
Wallace Wong
Wallace Wong is a Gender Identity Specialist based in Vancouver. He boasts that, of the 1000 children in his care, 500 are children from the looked after system. That is children who are, in some way, wards of the state. Wallace Wong works for the Ministry of Children and Families and also has a private practice.

He arrived at his current career path after noticing how many “transwomen” were impacted by the HIV/AIDs crisis. He initially began working with adults but soon noticed that the age of those with “Gender Identity” confusion was becoming increasingly younger.

You can listen to the full audio at this site. I imagine that many of you may diverge from their larger aims (as do I) however, given the dearth of coverage in other media outlets I will link to their research. This is the only way to honour my commitment to provide primary sources, where possible. The link is below.
The clips in my piece were included in the vimeo embedded in the above link. I have listened to it, in its entirety, and can attest to the accuracy of the transcribing. It is a long presentation and I can’t do justice to all of the issues it raises but below is a brief overview.
Wong argues that we must not confuse gender incongruence/roles with being Transgender but most of the examples supplied are of boys who like “girly” things. Expect lots of references to princesses and pretty things. He dismisses research showing high rates of desistance in children who, historically, claimed a trans-identity. He argues that “gender” is innate and quotes some research about hard-wired neurological causes based on MRI scans proving #LadyBrain. He also quotes some self-reported adherence to sex stereotypical behaviour, typically associated with the opposite sex. I suspect Wallace has not heard of the, Shakespearean, quote “the wish was father to the thought” (Henry IV, Part II). We are treathing retrospective wish fulfilment as if it is peer reviewed evidence. Laverne Cox & Caitlin Jenner are wheeled out to confirm the idea that children know they are trans age three. Caitlin, you may remember managed to father five children and win Olympic medals during his male life. Laughably, at one point a video commentator appears to think the existence of Facebook “genders” has some sort of evidential significance.


He is also at pains to dismiss any concern that confusion could arise between emerging homosexuality and a proto transkid. Similarly he argues that high rates of autism can be expected because both autistic traits and transgender traits are biologically determined. High rates of co-morbid mental health issues are to be expected, he argues, because being transgender is hard.

Below Dr Wallace seems keen that we should know he is seeing patients as young as 3. He also makes it clear about the fast pace of this change and the fact that research has not kept pace with this development.

Below is where Wong makes the startling admission that 50% (500 out of his 1000 referrals) are from the Ministry of Children and families. This means they are somewhere in the care system and commonly referred to as “Looked After Children”. Dr Wallace doesn’t appear to have much professional curiosity about the exponential growth in “transkids” over this period.
Jenn Smith (also based in Vancouver) is a male who expresses “feminine” and ascribes this to his experience within the care system. Jenn argues that children in care are particularly vulnerable to “identity” issues which also extend to “gender identity”. It was Jenn Smith who first made me consider this aspect of the debate.
You can catch up with Jenn Smith on his YouTube channel and here Jenn Talks specifically about this issue here:
Listening to Jenn Smith talk it is hard not to be concerned about an estimated figure of one in ten LAC (Looked After Children) identifing as transgender. This is contrasted with an estimated figure of one in 200 of children residing with their birth families. Another disturbing dimension is whether the indigenous children, over-represented in LAC settings, are also being medicalised as “transgender”. This has dangerous echoes of the scandal of sterilisation of indigenous peoples which is a stain on Canada’s history. If they are included in this population, of transkids, that is a damning indictment of those tasked with the welfare of children in British Columbia.
Wong does identify the dangers of social contagion in his presentation. I suspect this is now such an obvious phenomenon he feels obliged to address it. He prefaces the quotes below with some arguments that the internet has allowed “trans children” to develop an awareness of their identity and find acceptance, and knowledge, in on-line communities. Below, he at least acknowledges the dangers of kids, particularly those “on the spectrum” (referring to Autism I assume) to be swept along with trans-ideation.


Astonishingly he acknowledges that 20% of Transgender kids are autistic but this is simply dismissed because autistic kids and transgender kids are “born this way“. This is not an uncommon feature of arguments from Gender Identity proponents. Once you embrace the belief of an innate gender identity you can find evidence everywhere and fit facts to confirm your hypothesis. Conversely if, like me, you are a sceptic the ideology has more holes than a string vest.


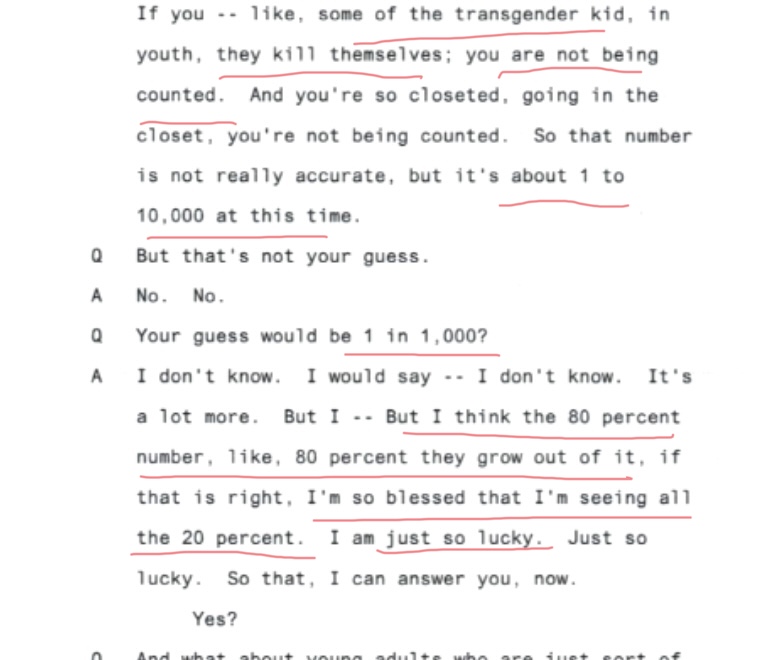
He introduces videos throughout his presentation and one is a parent whose child came out to them at three years of age. I have not included the parent’s quote but suffice to say, like a lot of these tales, it is a boy who likes pink and sparkly things. We are told that her original therapist counselled a watch and wait approach and quoted an 80% figure for expectations of desistance. The same presentation proceeds to rubbish a study based in the Netherlands which supported this observation.

What the audience are not told is that there was only one Gender Identity clinic in the Netherlands so the researchers made the, entirely reasonable, assumption that loss to follow up could reasonably be correlated with desistance. The alternative was that the child had been taken abroad, and paid for treatment, rather than access the free treatment within the Netherlands.
Wong also rubbishes another study which found that most of the boys grew up to be gay. The unfortunately named “Sissy boys” were identified for their Gender non-conforming presentation. Here Wong argues that the study was flawed because they did not use boys who said they were actually girls. It does not seem to have occured to Wong that it was the 1970’s. Identifying as the other sex was not a social norm at the time. It is the near ubiquity of teaching about Gender Identity in our schools (especially in Canada) that has left a generation thinking you can choose your sex.

Wong then utters this statement which shows he is utterly disregarding any research that suggests he may be making an egregious error. To much laughter he dismisses any caution with this facile statement. Apparently, if the 80% is correct he is lucky enough to be seeing the 20% who would persist. Crassly he also argues that some of those kids may not appear in the figures because they will have committed suicide. As I have said, many times, there is just no evidence for this epidemic of transgender suicides in adolescents. Wong may feel blessed and lucky but it was bad luck for any child who walked into his office.
All of which takes me to the more egregious aspect of the advice Wong is dishing out. The question of how to overcome barriers to access to Gender Identity treatment was raised. Wong requests that this part of his presentation is not taped and then, after a side swipe at the gate-keeping goverment, he advises: “Pull a stunt. Suicide, every time, they will give you what you need“


This series is looking at the vulnerability of Children in Care; who have no parents to speak up for them. Not all the parents in Vancover are absent. It was also Vancouver who imprisoned a father who opposed the provision of testosterone for his teenage daughter and refused to remain silent. It would be interesting to see who was the Gender Identity Specialist involved in that case. Is there a connection?

I could not say but I certainly want to do a series on parents caught up in this nightmare.
If you can support my work it will be appreciated. Below is one way to do so until we get more media outlets willing to cover the issues I cover on my blog. Only if it is affordable and regardless my content will remain free.
My next piece will be on the percentage of kids in care referred to GIDs, in the U.K. Are the researchers concerned that these, vulnerable, kids have no parents to question the medical interventions proposed? Or. Are they worried children in care are not being treated fast enough? Watch this space.

paypal.me/STILLTish
Researching Gender Identity Ideology and its impact on Women and our Gay Youth. Support is always appreciated (I have no income). All my content is open access so if you can’t speak publicly, and want to support those who can, only IF you have spare cash, this helps me keep going.
£10.00












 The ACLU have a proud history defending Civil Liberties and Free Speech. A legacy which has been utterly squandered by its advocacy of Gender Identity Ideology. As an organisation they appear unwilling to accept that Women, LGB people and even Transsexuals, have legitimate concerns about the extremist positions of Gender Identity Ideologues.
The ACLU have a proud history defending Civil Liberties and Free Speech. A legacy which has been utterly squandered by its advocacy of Gender Identity Ideology. As an organisation they appear unwilling to accept that Women, LGB people and even Transsexuals, have legitimate concerns about the extremist positions of Gender Identity Ideologues. 









 ⇒
⇒ Membes are instructed on use of
Membes are instructed on use of 








