Just leaving this here 👇

I have covered the BPS quite extensively. This is why Tania asked them the question. From their own guidance.

Examining Gender Identity ideology and its impact on Women's Sex based rights and Gay Rights. Exploring how this has taken such firm root in Western societies (Cognitive & Regulatory Capture).

Just leaving this here 👇
I have covered the BPS quite extensively. This is why Tania asked them the question. From their own guidance.
A letter in response to the guidelines. Reproduced, in full, below.
Numerous psychologists call for review of the BPS Guidelines for Psychologists Working with Gender, Sexuality and Relationship Diversity; plus response.

Following the response to J.K. Rowling’s essay ‘Reasons for Speaking Out on Sex and Gender Issues’ and the 18 June Newsnight report of safeguarding concerns at the NHS Gender Identity Development Service, we call for an immediate review of the recent BPS Guidelines for Psychologists Working with Gender, Sexuality and Relationship Diversity (BPS, 2019).
These guidelines state that a ‘gender-affirmative’ stance should be the default position adopted by psychologists. We are concerned that the instruction to ‘integrat[e] an affirmative stance into their model of practice’ restricts the use of many core models (systemic, trauma-informed, developmental) in formulating the factors resulting in the clients’ presentation. This places limitations on researchers and practitioners exploring the wider context of ‘gender’ and seeking to establish ‘best-evidence’ for the support of individuals with gender dysphoria.
For those unfamiliar with the guidance or discussion in this field, ‘gender affirming’ practice calls for psychologists to work on the basis that an individual’s belief in self-ascribed gender is ‘valid and legitimate’. We hope all psychologists value and respect the varied understandings that people hold of the world around them and of their personal experience. We suggest it is possible to value and respect a client’s experience, without taking a position of affirmation. Indeed we often do this within our work with various client groups. The BPS guidance stipulates that practitioners validate a belief in gender (both in general and in particular to the individual’s sense of self) without considering the evidence base in relation to the practice of belief validation.
Individuals who are questioning their identity with respect to their sex and gender clearly report significant levels of psychological distress. The long-term implications for this population resulting from the provision or denial of access to treatment are substantial. We recognise that appropriate, evidence-based guidelines are imperative to support the skilled psychological practice which our profession seeks to uphold. However, such guidelines can only be effective when these are the result of comprehensive research, conducted in an environment that supports free and independent enquiry.
In particular, we think it is imperative that psychologists are not prevented from using our core professional skill of formulation, exploring the origins and nature of distress rather than ascribing to one pre-determined ‘diagnosis’ or explanation. With other presentations we are in agreement that there are multiple contributory factors to psychological distress. It is only from this exploration that we can develop individualised formulations to guide our attempts to alleviate that distress. We think the current guidelines effectively prohibit psychologists from taking a questioning approach and applying ethical practice in these situations. The absence of a robust evidence base supporting psychological and medical intervention is a concern in this rapidly growing population, leaving significant gaps in our understanding of many relevant issues. The disproportionate increase in presentations of females to services, the phenomenon of so-called Rapid-Onset Gender Dysphoria, the voices of individuals who have desisted or detransitioned, and the experiences of those for whom existing treatments have been of value must all be addressed in the search for quality research informing best-evidence practice. Such research can only be conducted in an environment that is open to discussion in a respectful and professionally inquisitive manner.
We would like to see the current guidance withdrawn and the topic reviewed afresh in accordance with the rules of proper intellectual inquiry: the weighing up of evidence; the ethical considerations of psychological practice; and the avoidance at all times of ad hominem forms of argument. Some of the signatories below, with others, have submitted a formal request for the withdrawal of the guidance to the Society. We hope that readers will support our expectation that the freedom of expression of all psychologists will be defended, unambiguously and at all times, in relation to both research and practice.
Dr Katie Alcock (Senior Lecturer in Psychology)
Rachel Corry (Occupational Psychologist)
Ms Nina Gadsdon (Psychology Masters Student)
Dr Louise Fernandes (Clinical Psychologist)
Ms Pat Harvey (Guinan) (Former Chair of the Division of Clinical Psychology)
Dr Peter Harvey (Former Chair of the Division of Clinical Psychology)
Mr Ian Hancock (Retired Consultant Clinical Psychologist, Director of Psychological Services, NHS Dumfries and Galloway).
Dr John Higgon (Consultant Clinical Neuropsychologist)
Dr Anna Hutchinson (Clinical Psychologist)
Dr Gill I’Anson (Consultant Clinical Psychologist)
Mr Eric Karas (Retired Consultant Clinical Psychologist)
Dr Jeanie McIntee (Consultant Clinical & Forensic Psychologist & Psychotherapist)
Dr David Pilgrim (Former Chair of the History and Philosophy Section)
Julia Richards (Educational Psychologist)
Cas Schneider (Consultant Chartered Clinical Psychologist)
Karen Scott (Retired Educational Psychologist)
Dr Sarah Verity (Chartered Clinical Psychologist)
Dr Robert Watts (Clinical Psychologist)
Anne Woodhouse (Clinical Psychologist)
Colleagues who felt they needed to remain anonymous:
Consultant Clinical Psychologist NE England
Clinical Psychologist NE England
Consultant Forensic Psychologist S England
Clinical Psychologist NW England
Society response: We acknowledge that the BPS is a broad church, and there will always be differing views among our members on some issues. We are confident that our guidelines are based on the best current evidence and research in this important area, having been developed by experts working in the field. Clearly we share your concern about the safeguarding of children and young people, but our guidance is specifically for the care and treatment of adults, not children.
The draft guidance was sent out for Society-wide consultation on 19 March 2019. It was also sent to the Royal College of Psychiatrists, APA, BACP, BABCP, UKCP, Stonewall, LGBT foundation and COSRT for comment. At the close of the consultation on 12 April 2019 34 responses had been received. Just one of these responses mentions the issue of dissenting voices that is raised in your letter. This respondent also stated that the document was ‘well intentioned and positive’.
All our guidance is periodically reviewed. This particular guidance is the second version, having been revised in 2019. If there is a change in practice or evidence, then the need to revise the guidance would be established. In this instance, we will review the guidance if there are implications for the care and treatment of adults following the outcomes of:
As a Society we are committed to our members having a view and welcome different perspectives. As such any revised guidance will be sent out for Society-wide consultation and we would welcome your input into the revised consultation process.View the complete article as a PDF document
(Please note that some pictures may have been removed for copyright reasons)

If you are able to support my work please do so. I am unwaged and all my content is open.
Investigating the march of Gender Identity Ideology. The impact on Women’s rights and the cost paid by our Gay offspring & children on the Autistic spectrum.
£5.00
This is part 4 of a series on the British Psychological Society. This blog will examine the BPS treatment guidelines, from 2019. The 2012 version is covered in part three. The changes between the two versions are indicative of the level of mission creep. Unless otherwise indicated, all quotations are taken from this document. 👇
Guidelines for psychologists working with gender, sexuality and relationship diversity
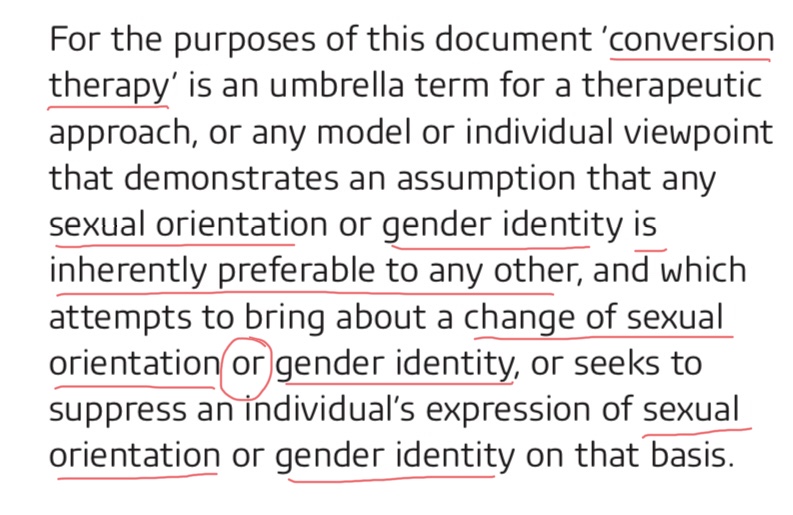
In Part One I looked at the background to a Memorandum of Understanding (MOU) that commits a number of organisations to reject Conversion Therapy
In Part Two I looked at the BPS position statement, on therapy pertaining to sexual orientation, and examined the profiles of the authors.
Part Three looks in detail at the recommended treatment guidelines and illustrates how far they stray from the impression given by the position statement.
The same names are involved, as were acknowledged in the 2012 version. You can find out more about some of these names in earlier parts of this series. Stonewall UK are also thanked for their help.


Gone are the warnings that caution is required before any irreversible medical treatments Ditto concern about the impact of Schizophrenia, or Aspergers, on Gender Identity Issues. The fact that most children/teens, with Gender Identity issues, will, turn out to be mainly Gay males and Lesbians has also disappeared. Why? What has changed?

What has survived are the ideas around Sexual Identities / sexual practices.

⇐ Here we see that the guidelines encompass gender, sexuality and those with diverse relationships. The phrase “assigned at birth“ is used, an ideological formulation to suggest it is not obvious in 99.9% of cases. Also “Cisgender”; another, contested, term claiming anyone comfortable with their biological sex is in fact content with their “gender”. As many of us point out, ad nauseum, accepting your biological sex does not mean you are comfortable with “gender” ! Especially since any definition of “gender” seems to be the based entirely on reductive sex stereotypes.
Moving on, here is a full list of what the BPS includes under “diverse relationship/sexual practices”. A veritable, word salad of queer theory inspired, nonsense.
 ⇒
⇒
The practice of BDSM is culturally specific and hardly a biologically determined part of sexuality. The claim this is all part of “human diversity” strongly implies all these “identities” have been with us since the dawn of time. A categorical falsehood which only survives by a historical revisionism, deployed by Trans Activists, which shames Stalin. Anybody who confirms that women,and men, have always rejected the constraints of expected gender roles is simply retrospectively transed.
 Membes are instructed on use of ⇒ ⇒⇒ preferred pronouns and warned not to stigmatise diverse sexual practices. Polite pronoun use is one thing, however, the use of “expect” and “correct” smacks of compelled speech and underlines how authoritarian this movement is.
Membes are instructed on use of ⇒ ⇒⇒ preferred pronouns and warned not to stigmatise diverse sexual practices. Polite pronoun use is one thing, however, the use of “expect” and “correct” smacks of compelled speech and underlines how authoritarian this movement is.
The dismissal of emotional problems and suicide attempts from this client group also seems dangerously lacking in curiosity, or research, into post-transition suicidality. ⇓

Minority stress is undoubtedly an issue for Gay and Transsexual/Transgender clientele. I think it is over-stating the case to dismiss all of these co-morbidities as arising from lack of social acceptance. Some victims of sexual abuse locate their involvment, in BDSM, as a response to these experiences or even how the abuse manifested itself. Some women talk of their involvment in sadomasochistic practices as arising from/causing negative impacts on their mental health and self-esteem. Some transsexuals refer to the mental stress of “imposter syndrome” and the relief garnered from naming, and accepting, their biological sex. The thinking underpinning these guidelines seems to prioritise an ideology rather than centre the client’s well-being. Sweeping all of these identities, sexual practices and relationship types into the prohibition of “conversion therapy” may deny therapeutic help to vulnerable groups. Not analysing underlying /subconcious motivations seems reckless. Yet, the BPS do exactly that: ⇓

Autogynephilia & Fetishistic Tranvestism
It is also significant that all reference to fetishistic transvestism has disappeared from this edition of the guidelines. Another notable, I would also argue tactical, omission is the phenomenon of Autogynephilia (AGP). This is a paraphilia and affects heterosexual men. The clinical description is that they have an “erotic target location error” and are aroused by the idea of themselves “as a woman”. An AGP male can derive satisfaction, sometimes overtly sexual, from invading female spaces. Is it any wonder that activists do not wish to draw attention to this type of transsexualism/transgender identity?

Here there is a brief mention of the mental health conditions which may play a role in a particular “identity”. This document is very keen to badge these as “extremely rare”.
Notice the shaming tactic of inferring any dissent is akin to racism.
The omission of the paragraph below, from the 2012 guidelines, is more transgender washing. Most people have no idea about autogynephilia, yet it is paraphilia documented for decades. It is also a condition for which men have sought treatment, rather than “transiton” . This begs the question of where they get this help when therapists simply affirm a trans identity.. This is also a tactical omission because acknowledging men adopting women’s clothing/identity, for erotic purposes, isn’t good public relations . Telling the general public, men with a sexual a paraphilia can safely be given to access women’s spaces won’t be appearing on David Lammy’s campaign literature any time soon. (Lammy is the UK, MP responsible for the passage of the Gender Recognition Act)

Too many policy makers are treating any male with a Cross-Sex Identity as if it magically transforms them, literally, into their chosen “identity”. This matters because we treat men, as a class, a certain way becauuse of the the statistical sexual offending rate against women.. There is no evidence this, changes “post transition” whatever that means no we are told it is transphobiv to expect a penectomy has been performed. In fact it sex offenders may, in fact, by higher judging my the males in the UK prison population. Moreover our politicians would know this if they had bothered to undertake any impact assessments. Instead they have shown a feckless disregard for women’s rights.
Gender Identity Ideology has gained such traction by the take over of bodies responsible for making policy and laws. Here the BPS calls for its members to become active in policy making and their community to “effect change” . The wholesale social engineering necessary to make organistations afraid to use the word “woman” dopt a whole new (dehumanising) language to describe us is not happenstance. Its indicative of institutional capture.

For emphasis I am including this next paragraph, even thought it is somewhat repeat some earlier points. Here the mandated belief is that sexual attraction operates based on “gender identity”. The wording is, I would argue, deliberately obfuscatory so it is not readily apparent that the BPS are actually de-coupling sexual orientation from sex. We have already been told that a male-sexed, and male-presenting person, can be a lesbian. Shouldn’t a therapist be able to explore what has given rise to this belief, because it is patently delusional. Is it ethicaly to endorse the boundary breaching this entails for the old fashioned kind of Lesbian. AKA WOMEN!
Below it is made explicit that no assumptions should be made about any medical interventions required, or undertaken. Once again, for emphasis, this is why more and more Lesbians and Gay males are starting to sound the alarm for what this means for their exclusive same sex orientation. This ideology parrots the idea that being “exclusive” in your, same sex, dating practices is “transphobic”. Does the BPS agree with this? What does this say about the legally protected characterisic of sexual orientation?

If you have not yet acquainted yourself with the idea of “Lady Penis” then now is the time because it is being taught in primary schools. See my blog below.
That is right. Your children are being taught that some girls have a penis.
This paragraph is also worth reproducing to the maximum size possible. Basically if an obvious man, who belongs to the male sex, tells you that he is, nevertheless, a lesbian it is your duty to accept this. Then again he may wish you to call him “slut” . This immediately makes me wish I knew the relative price comparison for a session with a psychologist versus say, a dominatrix.

Yep. I went there. Being call “slut” by a dominatrix is big in “femdom” and sissy porn. Website below takes you to a content warning that it is only suitable for over 18’s. You can get the drift from the promotional blurb.
Here is a review: {I had better not be involved in a crime BTW as my search history….}

Ths next paragraph I believe is referred to as a bait and switch. There is growing evidence of the abuse, of female partners, by trans-identified males with Autogynephilia. However this document emphasises that a transitioning partner should not feel inhibited in complaining about an accepting partner. I imagine this excerpt will draw a rueful grimace from transwidows. This excerpt also inverts the power dynamics in a relationship where only one is non-monogamous or practices BDSM. These two “identities”, it is implied, will be the marginalised/oppressed. Thus, in one fell swoop, the woman with a partner who has sex outside the relationship, or pays to visit a Mistress Kimberley, will be deemed at the losing end of a power differential with his partner. This is gaslighting in a gimp mask.

Finally. In the previous version of the guidelines much more time was given to the potential implications of irreversible medical interventions on children/teens. In this version we are simply told that “reproductive optiions…may be more complex”.

I have lost count of the times I have been flat out contradicted for saying we are sterilising kids when we put children on puberty blockers. We are. When you put children, as young as 10, on puberty blockers they invariably progress to cross sex hormones. They will be infertile. We are doing this in the UK.
Finally in my next blog I will make it clear there is opposition/concern within the ranks of BPS members.
If you are able to support my work please do so. I am unwaged and all my content is open.
Investigating the march of Gender Identity Ideology. The impact on Women’s rights and the cost paid by our Gay offspring & children on the Autistic spectrum.
£5.00
This is part 3 of a series on the British Psychological Society. This blog will examine the BPS treatment guidelines, referenced in the BPS position statement, covered in Part Two. Unless otherwise indicated, all quotations are taken from this document. 👇
In Part One I looked at the background to a Memorandum of Understanding (MOU) that commits a number of organisations to reject Conversion Therapy. The concern I have is the MOU to oppose “conversion therapy” includes both Sexual Orientation and Gender Identity. An unintended consequence is gay males and lesbians may be placed on an unnecessary medicalised pathway to “transition”. Ironically this is actually a form of Gay Conversion. Therapists should be able to prioritise reconciliation to biological sex/sexuality as the ideal outcome. Same sex orientation doesn’t involve lifetime dependence on cross-sex hormones/surgery. This MOU effectively bans therapists / parents from affirming biological sex and sexuality.
In Part Two I looked at the BPS position statement, on therapy pertaining to sexual orientation, and examined the profiles of the authors. The BPS statement mentions “gender identity” only in passing, yet the full guidelines centre Gender Identity issues as much as sexual orientation. This has all the hall marks of yet more “stealth” activism.
Part Three looks in detail at the recommended treatment guidelines and illustrates how far they stray from the impression given by the position statement. Even the title deviates from a focus on Sexual Orientation: “Psychologists working therapautically with Sexual and Gender Minority Clients”.

Christina Richards is employed at the Gender Identity Clinic (GIDs) sometimes, informally, referred to as the Tavistock. You can read about Christina here. Richards has a very high profile in the field of Gender Identity and especially in organisations which promote an “affirmation only” approach to Gender Dysphoria. :https://christinarichardspsychologist.wordpress.com/
Christina may also be remembered for defending a job advert which sought to recruit more people to work at GIDs and included this memorable part of the selection criteria:

Polly Carmichael is the director of the Gender Identity Service (GIDs) as I write. Penny Lenihan is also a psychotherapist based at GIDs. Meg Barker (now Meg-John) is an activist who campaigns on Bisexual issues and was the author of a bat-shit crazy document for the BACP (British Association of Counsellors and Psychotherapists). She campaigns for the recognition of those practicing BDSM/Kink /polyamorous relationships. Meg also thinks Bi-sexuals are stigmatised by the assumption that they are involved in diverse sexual practices. She/He/They/Zie (who the hell knows/cares?) states that the “bi” in “bisexual” is problematic as it suggests there are only two genders. Of course, sexual orientation is described, as same gender attraction which, as we now know, is not synonymous with biological sex. This has the effect of undermining Same-Sexual Orientation. (See later definition of “lesbian”)


Note also contributor Christine Burns, a prominent Trans Activist and editor of a collection of essays, in the book “Trans Britain”. Also Stephen Whittle, who obtained law qualifications, to better advocate for trans rights. These two names crop up numerous times, both are “trans”
Here is a flavour of what the authors mean by “sexual identities”. It is not, as you may have expected, a reference to different sexual orientations. It includes sexual practices such as sado-masochism, transvestism as well as the more benign sounding asexuality.

The BPS document is very clear it includes “Fetishistic Transvestism” as shown by the quote below. Bear in mind that transvestites, now referred to as part-time cross-dressers, are officially under the Trans Umbrella, according to Stonewall UK. I wonder if this definition will appear in the 2019 version of this document? The protection of “sexual minorities” is now extended to people with a paraphilia, and by people I mean men. Remember this when you tweet out vacous statements about supporting people to “live as their authentic self”. I am pretty sure most people don’t realise this is what we are being asked to sign up to…. Did the MOU signatories?
Here we are reassured that not all of the cross dressing men, now officially transgender, are fetishistic. Once again women cry: “How do we know which one’s?”. Remember single sex spaces are not because all men are predators but because a minority are. The same applies to men. who identify as transgender. How do we know which part of the umbrella they come under? Too many policy makers are treating any male with a Cross-Sex Identity as identifying as if this magically transforms the statistical sexual offending profile to literally equate to that of natal (for emphasis only) women. There is no evidence of this, quite the contrary.

Another aspect of Gender Identity Ideology is the integral notion of power relations between “genders”. The notions of dominance and submission are necessary for sexual power games. The only subversion here is sometimes the sexes get to “play” different roles. The hierarchy remains intact but, gender identity ideologues argue, this somehow undermines “gendered expectations” and liberates us all! BDSM normalises the notion of pain, submission and servitude. To get an idea of just how liberating this has been, for women, find me a man who has died at the hands of a woman who then used then used the “rough sex” defence to avoid prison. Doesn’t happen.

To get a further idea of just how regressive this is let me quote an excerpt from a Master’s thesis. It was written by a man who documented how BDSM helped cement his identity as a transwoman. He had an unpleasant, sexual, encounter where his safe words were disregarded by the other participant. This is what he took away from that encounter:

Naturally Queer Theory proponents avoid the unpleasant truth about prostituted women. Despite the fact clients are practically always men and the percentage of male prostitutes, also servicing men, are dwarfed in comparision to the females. The clinicians are warned about pathologising issues such as sex addction and pornography use.

In an outbreak of honesty they do, briefly, acknowledge there is a body of work (See Gail Dines) on the objectification of women in pornography.

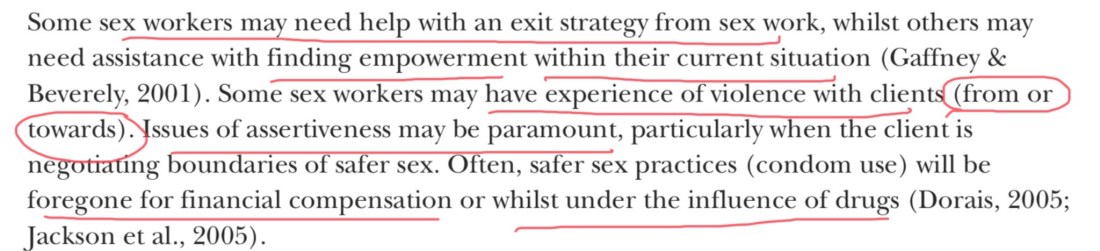
The centrality of pro-prositution arguments within Trans-Activist ideology is indicated by the two slurs used against women, who question this belief system. These are Swerf and Terf, acronyms for Sex Worker/Trans Excusionary Radical Feminists. Some radical feminists are ex prostituted women who remain deeply concerned for the women who remain in prostitution. Others are opponents of the sale of women’s bodies and care deeply about the women labelled “sex workers”. Here the BPS pay lip service to the women who need an “exit strategy” . (What work requires an exit strategy?) but shamefully tries a “bad on both sides” argument re the perpetrators of violence. Even worse it suggests the “sex workers” need a route to empowerment and to learn to be assertive. Shame on everyone who agreed with this paragraph.
The centrality of pro-prostitution narratives is striking in prominent Trans activists and Celebrities. Janet Mock saw prostitution as a good way to validate their “womanhood”. Mock even compared prostitution to the underground railway that enabled Black people to escape the South and Slavery. Seeking male validation of your womanhood, via prostitution, runs counter to feminist campaigns to reject our commodification/ objectification. Yet another example where the “feminist” agenda of ,self-described, Transwomen, actually undermines women’s position in society. It is almost as if the interests of the new kind of women are perfectly in tune with men’s rights and diametrcally opposed to the interests of women.

I have seen many sad stories about gay males entering prostitution to fund their flight from their sex and sexuality. I have not seen any voices expressing concern about the rate of prostituted males killed in countries like Brazil. We see lots of concern about the deaths of transwomen but very little acknowledgment that their deaths are related to the prostitution industry which has a a high rate of violence and death. Not so much empowering but devouring this demographic. Clients are overwhelmingly men despite the attempt to pretend there is a high demand from women. I think the Chicks with Dicks phenomenon is likely near as dammit 100% male.

I include this quote just to note that the theme of Lesbians changing their orientation is recurrent.

Here the BPS gives the word “lesbian” to males, who present as male, but describe themselves as “lesbian”. To all those people denying this is actually happening. Here is yet more confirmation.

The BPS also endorse the idea that sexuality is fluid. While there are complex debates around whether sexuality is innate and unchanging one of the key victories in Gay Rights movement was that their sexuality was fixed and therefore Conversion Therapy should not be attempted, and moreover, it won’t work. However this doesn’t chime with the idea that a Lesbian can express their sexuality with a male-bodied “lesbian”. Is this why the idea of a fluid sexuality has gained ground in advocates of Queer Theory?

Here the BPS explains that an absence of socialisation related to your preferred gender may mean that trans people have difficulty with their “gender performance”. That may explain the lingering male socialisation that generates so many woman-identified people threatening women with their male genitalia. Very interesting use of the word “performance” here. Performative femininity is something feminists have sought to resist and reject illustrating, once again, that it runs counter to women’s liberation for our sex to be reduced to simply an “identity”.

I would love to see some research about the long term mental health impact of pretending to be something you are not. The Imposter Syndrome must be debilitating and I cannot imagine it is psychologically healthy.
Therapy or Social Engineering?
Another interesting observation below. Yes! There are people who are fine with all sorts of personal self-expression and not conforming to expected sex stereotypes should be supported. The next sentence is fascinating. Ideologues insist that young people should be encouraged in this, regardless of personal cost, because it aids the “deconstitution of the gender binary”. That doesn’t read like a careful, therapeutic approach to clients with “Gender Dysphoria”. It reads as an appeal to harness them as activists for a wider project of social engineering. Is that even ethical?

Medical Interventions for Gender Confusion.
The quote below contains an important acknowledgment of research which highlights that the majority of “gender atypical” youth will be young gay males/lesbians. It also stresses the it is “imperative irreversible medical decisions should not be made“. This document is therefore not reflective of a purely affirmative model and thus gives contradictory messages. It is also interesting this comment survived the edit , though the BPS go on to advocate stopping puberty and early surgery. How clinicians were supposed to navigate these mixed messages is a mystery to me.

The document also raises some concerns which are echoed by those of us concerned about the impact of Gender Identity ideology on gay males and Lesbians. Here Clinicians are warned about the cultural context surrounding sex stereotypes. They raise the issue of father’s who may be concerned that they have a “sissy” for a son, we could call this homophobia. Again they also highlight that the majority of pre-pubertal children desist and later identify as gay or bisexual. I will be very surprised if this survives the BPS guidelines for 2019.


Furthermore it goes on to acknowledge the treatment for Gender Identity Disorder (previous name for Gender Dysphoria) is “experimental”. Note that by 2011 GIDS had already begun blocking puberty for children as young as 10. A decade later they still have not published the research outcomes from that “Study” ,despite being obliged to do so. I use inverted commas here because I am not the only one who feels this “study” was a pretext for embarking on the early medicalisation of gender confused kids/teens. We are starting to see some of the fall-out from this approach in the emerging phenomena of de-transitioners.

Another series of startling admissions echo the experience of parents dealing with our Gender Dysphoric kids/teens. Clinicians are warned that an obsession with changing sex may arise due to schizophrenia or Asperger’s syndrome. They also warn about the role of the internet in fostering a trans-identity. Furthermoe they caution people of the consquences of advising people who you do not really “know”. Anyone who has visited the Trans related subreddits will see that this sort of “coaching” is a regular feature of that forum.


Even more worrying is the growth of on-line Gender Identity services who are facilitating the dispensing of hormone treatment. These operate on the “informed Consent” model which basically hands the treatment decisions to their “clients”. Basically these practioners discourage any gatekeeping (caution) and agree that a “Trans” person knows their gender identity best. It is therefore the role of the clinician to “affirm” not “question ” a client’s Gender dentity. The caution expressed below seems to have all but disappeared in modern practice.
Below they highlight that trans individuals may “embellish or limit personal history information in order to obtain desired treatments”. Parents are well aware that our offspring re-invent the past and, in my opinion, this is one reason why we are demonised and sidelined. When our offspring claim to have always felt like the opposite sex we are the people who can offer a counter-narrative based on facts.

Here they present a list of the surgeries that may be on the list to enable people to “live as their authentic self”.


If you are able to support my work please do so. I am unwaged and all my content is open.
Investigating the march of Gender Identity Ideology. The impact on Women’s rights and the cost paid by our Gay offspring & children on the Autistic spectrum.
£5.00
For the purposes of this blog I am interested in how the British Psychological Society (BPS) came to draft the Memorandum Of Understanding (MOU) outlawing the practice of Conversion Therapy. I have revisited their pronouncements from 2012 to trace what led up to the BPS stance. First I looked at the summary document which doesn’t give much away. You can read this here: 👇
BPS Positions Statement on Therapies Attempting to Change Sexual Orientation (2013)
This document is dated December 2012 and it’s title is reassuring. Clear statement that the BPS is concerned with Sexual Orientation. No conflation of sexual orientation with Gender Identity.

Indeed the short document is focussed almost entirely on opposing conversion (sometimes referred to, sinisterly, as “reparative”) therapies relating to sexual orientation. Only this one sentence references “Gender Identities”.

If I had read only this position statement I would have assumed the BPS were still talking about Gay Conversion Therapy. If I was a stealth advocate of Gender Identity Ideology the above quote provides enough “plausible deniability” against accusations of duplicity. The authors can argue they referenced gender/identities in the summary document. Anyone not versed in Trans rhetoric, (who was in 2012?) would not have picked up the reference to “gender” and “identities” or the wider implications. I wonder how many BPS members read the full document to which they refer?
The authors allude to a 100 page guidance which sets out, in detail, the expected treatment guidelines that Therapists are expected to follow. If you didn’t go on to read this document you would be unaware of what you were actually signing up to…

I will cover the above document, in detail, in my next blog. First I want to have a look at the people, publicly, involved in producing the BPS position statement. If I have learned anything, from my deep dives into Transgender Ideology, it is that the same names recur. It is chilling because a tiny minority of activists have managed an astonishing level of cognitive and legal/policy capture.
Here are the named contributors to the BPS position statement.

Dr Lyndsey Moon (Chair)
Here is a profile of Dr Moon which makes it clear their interest in Queer Theory pre-dates this position statement by many years. https://www.beeleaf.com/beeleaf-team/igi-lyndsey-moon/

Here Dr Lydsey is referenced in relation to a meeting with the Government Equality Office, in July 2019. Note their attendance was by invitation of the GEO.

Below is the website which details the meeting with the GEO and also introduces another group : Psychotherapists and Counsellors for Social Responsibility (PCSR). Well worth reading this because they report that they felt “heard” and clearly have on-going contact with senior figures within the Government Equality Office.
https://www.pcsr.org.uk/resources/13
The link above also provides full details of the LGBT Advisory Panel to the GEO. Note the name of Dr Michael Brady LGBT advisor. The panel of LGBT advisors which includes Ruth Hunt (then CEO of Stonewall), Paul Dillane of the Kaleidescope Trust and Paul Martin of Consortium. This LGBT panel was expanded in membership later and included James Morton of Scottish Trans Alliance. The LGBT Advisory panel, to the GEO, is also crying out for a full analysis of it’s compositon and its activities.
By August 2020 Dr Moon appears to have a multiple identity as Dr Igi/Lyndsey Moon. Here she/he/they (who knows?) speaks fluent Gender Identity speak encompassing the gender fluid, the non-binary and their right to equal treatment (fair enough). The group also campaign for these identited to be protected from “conversion” therapy. Most people are aware of the shameful history of Conversion attempts of homosexuals. The literature on conversion attempts of the “Gender Fluid” and “non-binary” community is something with which I am much less familiar.

Dr Moon is also now the chair of this organisation to campaign against conversion therapy:

Dr Joubert is another author who works in the field of Gender Dysphoria/Transsexualism. He provides diagnostic services to enable access to HRT (cross sex hormones) and surgeries. He also provides documentation to support applications for a Gender Recognition Certificate. He has also worked with Transgender prisoners. He is deeply entrenched in the Gender Medico-Industrial Complex.

Dr Pestano works in the field of Gender Dysphoria though his main focus seems to be Aspergers/Autism. 
Estimates of the percentage of referrals to Gender Identity Clinics, with a diagnosis of Autism are up to 30%. Females with autism are less likely to have a diagnosis so the prevalence of diagnosed females, in Gender Identity Referrals, should raise alarm bells. Dr Postano may very well be aware of this and his therapy may be perfectly appropriate. I would, however, like to see more experts on autism raising some concern about why so many autistic kids are identifying as “transgender”.
You can watch Dr Joanna Semlyen and Dr Moon speaking to parliament on LBGT mental health in May 2019. In it you will find references to Bridging hormones which is the practice of providing cross-sex hormones to those on the waiting list for Gender Identity Clinics. Lots of references to hetero-normative, different identities, non-binary, gender fluid etc. Dr Semlyen makes a plea for the inclusion of gender identity and sexual orientation in databases to make LGBTQ+ people feel confident in their acceptance. It’s not clear if Dr Semlyen advocates for sex to be replaced with “gender identity” but we now know this is already happening. The other panel member says acceptance is not enough. People with different identities should not be simply accepted they should be celebrated. One of the contributors is quoted saying the following: “LGBTQ identities should be very highly valued, not just equal, not just part of the mainstream, but much more valued”. It’s almost as if they have no concerns that they may be fuelling a backlash against the communities they purport to serve.

You can watch this session below and read the full transcript of the evidence. All via Hansard.
Or read the transcript Oral evidence – Health and social care and LGBT communities – 15 May 2019
Notice that Sarah Champion makes every effort to make sure the topic of trans suicides comes up. Suicide Ideation / attempts crops up frequently in this “debate” using statistics which have been debunked many times. I mention this because Sarah Champion has been challenged , my myself and others, due to her use of suicide statistics which inflate the risk to transgender teens. I wish politicians would do some due diligence and pay attention to Samaritan’s guidance on responsible coverage of suicide risk. I cover this here: Suicide in the Trans Community
Most people will, instinctively, wish to see Gay Conversion Therapy banned. Lobby groups know this so they are using stealth tactics to bolt on “Gender Identity ” to a popular cause. As I have argued, consistently, this legitimises the new Woke Gay Conversion Therapy. Activists argue that failing to adhere to sex stereotypes may mean you are born in the wrong body. Non-adherence to sex stereotypes is common, especially in Gay males and Lesbians. One from the rise outcome of Gender Identity Ideology is Lesbians and Gay males are, once again, hearing “born wrong” narratives dressed up in a rainbow costume.

This forced teaming, of the T ,with the LGB, has proved a disaster for homosexuals. in so many ways. Gender Identity Ideology threatens to undo the many victories of Gay Right’s activists In The Denton’s Document, Lobbyists for Gender Identity legislation are encouraged to latch onto popular legislation to sneak in further entrenchment of Gender Identity Ideology. Gay Conversion Therapy bans, which include “gender identity“, are no exception. I will link my piece on the Denton’s document here, Everybody should read it, 👇
In this blog I am simply looking at the BPS position statement. I will follow this up with the a look at detailed guidance to which we are signposted. It is over 100 pages long in this edition and this article gives you a good idea of the kind of content you can look forward to from the BPS……


For the purposes of this blog I am interested in how the British Psychological Society (BPS) came to draft this Memorandum Of Understanding (MOU) outlawing the practice of Conversion Therapy. I imagine most people will, instinctively, see this as an unmitigated good but beware. As I have written in my blog below stealth tactics are in play. This is not just about Gay Conversion Therapy. it also includes “Gender Identity” which makes it a very different proposition. This is a tactic. See my post on The Activist’s play book below:
Activists are encouraged to latch onto popular legislation to sneak in further entrenchment of Gender Identity Ideology. Gay Conversion Therapy bans, which include “gender identity“, are no exception.
Here I am simply looking at the MOU but I will follow up with blog on the BPS guidelines, referenced in this document. 👇
memorandum-of-understanding-v2-reva-jul19
First up a definition 👇 as provided, in the MOU, which you can read below
For regular readers you will know my concern is “affirming” a Gender Identity, at odds with your biological sex, may very well be a form of Gay Conversion Therapy. I cover this below.
The Woke Gay Conversion Therapy?
The BPS sets out its stance in this document. Sexual orientation is defined such that anyone whose “Gender Identity” is at odds with their biological sex is not excluded from the target of their sexual orientation. It paves the way for male lesbians and female gay men. It also includes asexual as a sexual orientation which is starting to become more prevalent in communications from the likes of Stonewall U.K. (For overseas readers Stonewall is a UK organisation which, historically, fought for Gay rights). The BPS also have signed up to the belief that sex isn’t binary despite the fact that we are a sexually dimorphic species. Sigh!

Next, clip below, BPS members are told they are not allowed to favour any Gender Identity over another. The language is obfuscatory. The BPS doesn’t support therapeutic approaches to reconcile a child /youth to a Gender Identity that aligns with their biological sex.The BPS effectively supports only a Gender Identity at odds with biological sex. How else will they disrupt the Gender Binary and queer social norms? Queering society turns out to have meant straightening the Gays. Who knew?
It is my, unashamed, preference that my son reconciles to his sex and sexuality. In an ideal world our offspring will live a full life, in their sexed body, with whichever sex forms the basis of their attraction. This means they won’t depend on cross sex hormones, for the rest of their life, or face unnecessary surgical procedures. This is the ideal outcoe and this should not be a controversial statement. What other area would parents be called bigots for wanting their offspring to reconcile to a healthy body as a first line of “treatment”? Or to be comfortable with their same sex orientation? We are living in the upside down.
Notice the quote, below, also includes the sentence includes both “Gender identity” and “Gender Expression”. I have yet to see a satisfactory, definition that explains why these terms are deemed to describe distinct phenomenon.


The MOU does state that it is permissible to access therapy to reconcile conflict about your sexuality, or gender. The question is how is this possible if therapists are too afraid to explore it? This doesn’t square with the idea it is harmful to seek the path of least medicalisation. Being gay doesn’t set you on a lifelong dependence on #BigPharma it also doesn’t mean you are born wrong, and definitely not in the wrong body. The exemptions the BPS do emphatise, below, are in respect of exploratory work to enable “trans” patients to access hormones or other medical treatments. Why no similiar exemption for patients who may be having trouble accepting their homosexuality?

Next up I will look at the guidelines quoted below. I have had a sneak preview of the latest ones and an earlier guide from 2012. In 2012 the summary guidance is scant on details. However both the 2012 guidance and the 2017 (updated 2019) are clearly driven by the involvement of prominent Trans Activists / proponents of Queer Theory. It appears to have taken less than a decade for the BPS to go full Gender Identity ideology compliant. The details of the guidance will be on my next blog which lists the many familiar names who have corrupted the BPS.

Here are a list of the signatories. I will just pick out a few. Jay Stewart, from Gendered Intelligence jumped out: A keen proponents of Queer Theory /Gender Identity Ideology. Gendered Intelligence are infamous for producing a guide to trans sex, for youth, which contained this gem.

I could have sworn it was Gendered Intelligence which produced a guide, to terminology, which claimed “vagina” for “transwomen”and relegated women’s vaginas to “front holes”. I couldn’t find that clip but if anyone has it let me know and I will add it.
The British Association for Counselling & Psychotherpy (BACP) also signed. The BACP regulate University courses in this area so Universities have to comply or they won’t have their courses accredited. The BACP also published a document which seemed to have difficulty including working class women, from the North of England, in their definition of a female gender identity. For more on this look at the #TransNorthern on twitter. We women, of the North, had a lot of fun with that one.
More worryingly, one of the signatories was the Medical director of NHS England. .

And here are the final signatures together with their supporters and it includes union members and the Royal College of Genderal oops General Practitioners. 


paypal.me/STILLTish
Researching Gender Identity Ideology and its impact on Women and our Gay Youth. Support is always appreciated (I have no income). All my content is open access so if you can’t speak publicly, and want to support those who can, only IF you have spare cash, this helps me keep going.
£10.00



