Part 6.
This paper was referenced in part 5 of this series. You can read part 5 here: 👇
PDF of the paper below: 👇
The paper was published, in November 2020, in the Journal for Child and Adolescent Mental Health.


This paper is jointly authored by Anna Hutchinson and Catherine Butler. Dr Butler is an academic, based in the psychology department, at Bath University. Dr Hutchinson has impeccable academic credentials and has held senior, clinical, posts including a stint at the Tavistock centre. 👇
LACK OF DATA:
The common theme in all the pieces I have done, on the topic of detransitioners / desisters, is a lack of current data. Desistance rates have, historically, been found to be as high as 98% for children who present at Gender Clinics. Even a desistance rate of 85% should call into question the practice of giving Puberty Blockers to children. Which, let me remind you, in the United Kingdom, are given to children as young as 10.

We also know that over 98%, of children, given puberty blockers, progress to cross-sex hormones (CSH). This suggests we lock these kids into a medical trajectory. Trans-activists argue the near ubiquity of progression to cross sex hormones is evidence of solid diagnostic criteria; which I find implausible. Here a Clinician, from the Tavistock, admits uncertainty adding that this is why it is important to get the parents to take responsibility for putting a child on puberty blockers. 👇 ”Because we dont have the evidence base” . {Dr Aiden Kelly}.

The near certainty these kids will progress to CSH also undermines the argument that blocking puberty allows a ”pause” for the child/family to weigh up their options.
Detransition Denial.
Rising rates of referrals to gender clinics is a worldwide phenomenon. There is also a concomitant rise in detransitioners. At the same time there is a widespread reluctance to acknowledge desisters/ detransitioners. The authors speculate, correctly in my view, that the dismissal of detransitioners’ testimony is driven by fear; a fear their stories delegitimise medical responses to Gender Dysphoria. This, I would add, threatens the profits of the Gender Industrial Complex. Suppressing information about post-transition regret, in this cohort, distorts the evidence available to judge the success rates of medical transition. It also doesn’t allow for any, evidence led, improvement in diagnostic criteria by identifying commonalities in the detrans community.
Furthermore disregarding detransitioners means medical professionals are poorly equipped to deal with regret. There is currently no guidance to address the consequences of post ”transition” regret; whether psychological or medical.

GENDER JOURNEY:
Despite the reluctance to acknowledge this community it has become increasingly difficult to deny post-transition regret. Some transgender activists now, implicitly, acknowledge the phenomenon but claim this is all part of a “Gender Journey” . This paper uses similar language, below, calling it a “development trajectory”. I am extremely wary of this framing which smacks of spinning regret for public relations purposes. It is, nevertheless, the case that some detransitioners say they may have been left with doubts had they not tried medical transition. However, we shouldn’t discount the possibility these responses are driven by a, subconscious, desire to salvage something positive from the experience. Either way I think we need to be cautious about this language which may serve to mask bad diagnostic techniques and normalise regret as an acceptable outcome.
HOMOPHOBIC BULLYING:
As with the other studies I have reviewed, the experience of homophobic bullying is identified as a factor leading to adoption of a trans-identity. We could see this as a mal-adaptive coping mechanism. The other recurrent themes are isolation; poor peer relations and family difficulties. Factors which appear related to desistance also recur. Understanding commonalties in desisters could also assist with better screening of those who present at gender clinics. This cautious approach has been cast aside with the current ”affirmation only” policy; which is being rolled out in new pilot clinics under this government.

The authors are keen to highlight research that stresses the importance of family support for “transitioning” . They also suggest the corollary can be feelings of shame, if the outcome is regret and re-identification with birth sex. In fairness parents, like me, who think our teenagers are making a mistake, may find our children are similarly inhibited from expressing regret. There is a natural reluctance to confirm your parent’s were right and admit you made a mistake.

The authors point out the development of diagnostic criteria, for children, is a relatively recent development. This allows trans-activist to argue earlier cohorts may have swept up children who were merely ”gender non-conforming”. This argument is used to dismiss earlier research, showing high rates of desistance, as historic failures in diagnosis. Trans-activists argue that diagnostic techniques have improved and earlier data is not relevant to the current cohort. I am cynical about this argument.

LOSS TO FOLLOW UP:
Some key themes about difficulties with research on detransition are covered below. Those who regret the treatment they received are less likely to return to the clinic who they may feel harmed them. Loss to follow up is a major stumbling block to getting accurate data. Worryingly the length of follow up times is quite short. If, as Dhejne says, we are looking at an average of eight years, before regret emerges, we are only at the beginning of this wave of detransitioners. Given there are already over 23,000 in the detrans reddit forum that is horrific to contemplate.

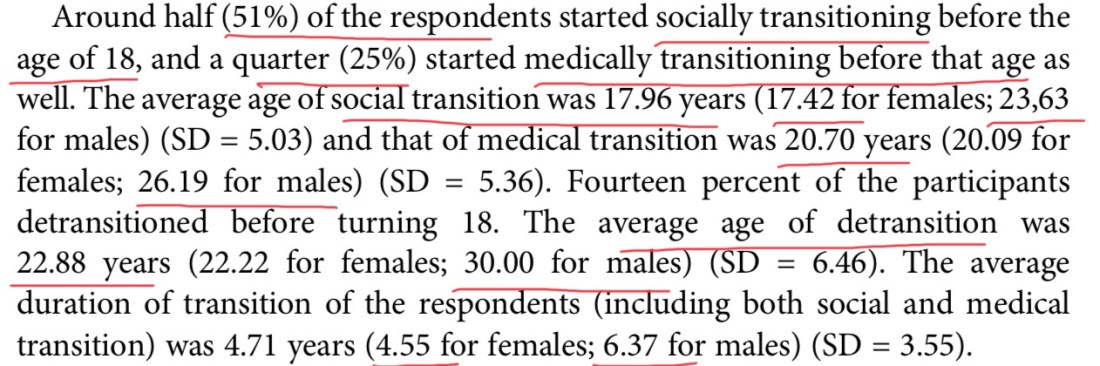
CHANGING DEMOGRAPHICS:
This section is critical in understanding the changing demographic referred to Gender Clinics. The scale of referrals; increase in females; emergence of different types of identities; the impact of socially transitioning children as well as the phenomenon of teenage onset gender dysphoria are all salient factors.


Our understanding of the above phenomena is limited and yet clinical practice has embraced an affirmation model with seemingly little reflection.
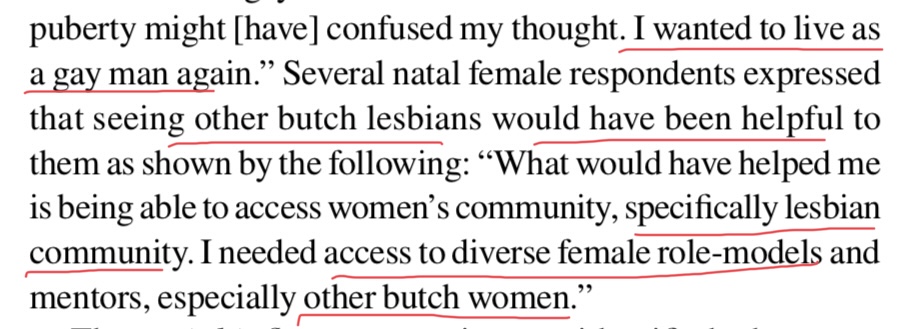
AUTISM & HOMOSEXUALITY
Autism and same sex attraction are features of the current, young cohort and we should all be heartbroken so many don’t feel comfortable with their homosexuality. It is for this reason that I describe what we are doing as a from of Eugenics/Gay Eugenics.

Clinicians will need to develop a whole range of different skills to deal with the emerging cohort of detransitioners. Some may have undertaken medical treatment which means they can no longer produce the appropriate hormones for their sex. Young women who can no longer have children may need counselling. As covered in my previous piece many detransitioners were very critical of the inability of psychologists and doctors to address their needs.

I doubt a young man who emerges with no testicles/penis or a female with no breasts/womb would regard this as a period of creative exploration. 👆
The advice below is likely appropriate for therapeutic approaches to working with clients. I also argue, we should be extremely wary of introducing permanent, medical intervention whilst, simultaneously, paying lip service to the idea of ”gender fluidity”.

I also object to the idea that we accord the description of ”acceptance” to the families going along with the idea our children should become medical patients for life. The parents who are supportive of our gay offspring, and their variant expressions of masculinity /femininity, are the ”accepting” parents.
The paper presents some practical advice for clinicians who are increasingly likely to encounter detransitioners. I would add that doctors who have prescribed treatments, which have resulted in regret, will need guidance and support. They may be defensive in their response to detransitioners who could be very angry. Detransitioners have identified peer support as invaluable and clinicians need to be aware of the networks available.

The themes emerging from the growing body of research on detransitioners make it clear we need to start looking critically at medical responses to a psychological phenomena. We should stop normalising permanent dependence on synthetic hormones/ surgery on healthy bodies. We need to face up to the real regret we are seeing and stop cloaking a medical scandal in the language of ”Gender Journey” or using phrases like ”creative exploration”. If gender is fluid why are we accepting permanent interventions for children and teens?
Guilting families into going along with this by applying the term ”acceptance“ to “affirming” parents is emotional blackmail. How is agreeing your son /daughter needs hormones and surgery, to be authentic, acceptance? Surely it is the exact opposite?
CONCLUSION:
We need more research to better predict outcomes and develop guidance so clinicians know how to deal with the needs of detransitioners. Work to understand this new demographic is still in its infancy. Once doctors have to face the consequences of post transition regret maybe this will re-engage their critical faculties. Right now I see only reckless endangerment.

I do this full-time and have no income. If you want to support my work, and can afford to do so, here is one way.

Researching the impact of Gender Identity Ideology on women & girls as well as the consequences for Lesbians, Gay males and autistic kids. I do this full time and have no income. All my content is open access and donations help keep me going. Only give IF you can afford. Thank you to my generous donors.
£10.00