Contrary to my usual practice I cannot link a PDF here. Below is the on-line link to the paper. It is open access but download and print are disabled.
Paper on detransition
Some of you may be familiar with The author, Kirsty Entwhistle. She is one of the Tavistock whistleblowers and was, previously, based at their Leeds branch. You can read Kirsty’s open letter raising her concerns here:
Open letter to GIDS
My son was referred, aged 19, to the Leeds branch of the Tavistock, last year, by my own GP. I have no way of ascertaining who prescribed the cross sex hormones he obtained, just six weeks later.

Yet another clinician raising the issue of detransitioners while the government seems committed to legalising the Woke Gay Conversion Therapy under the guise of banning it. 😳. The abstract references another paper which called for empirical research on desistance and detransition. The new demographic, referred to Gender Clinics, have been documenting their experience in support forums for those who know this was a mistake. It is now urgent that we record the detrans experience, from anecdotal, to clinical research. Thankfully this is now starting to happen.
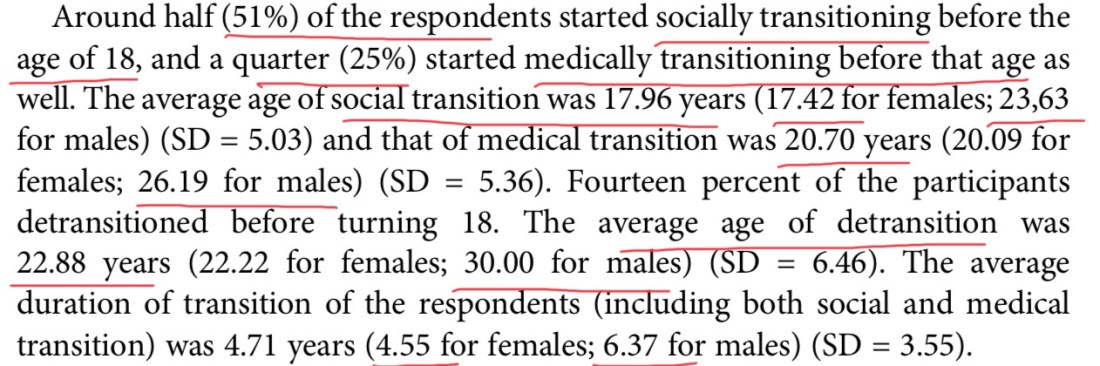
Here is the abstract to Kirsty’s research.

I will see if I can get access to the Butler Hutchinson paper, in full, to add to this series. For those of you with access, to the Journal for Children’s and Adolescent Mental Health, here is the link:
Butler and Hutchinson
As with the other pieces in this series the call is for some formal academic papers to capture the experience of this cohort and commence systematic follow up of outcomes. Gender Clinics seem to have determined that their role does not require formal tracking of *all* their referrals. They need to be compelled to do so they can evidence that this ”treatment” relieves Gender Dysphoria and that medical responses are the only way to alleviate the distress. The decision making process of teenagers and young people also requires more consideration; given how many detranstioners state they did not feel fully informed.
We need a shift in clinical practice to address the root causes of this bodily disassociation rather than funnelling sufferers down a medical pathway.

Those of you on twitter may be aware of Claudia Maclean. This is Claudia’s story as covered by Julie Bindel, in 2007. Claudia continues to speak up for our gay youth, for which I will be eternally grateful. I want a world of true diversity where a gay boy, like my son, with all his variant presentation of masculinity is free to be himself. I do not want a world where he is coaxed into a faux-straight, medicalised closet before he can enjoy a fulfilling, sexual, relationship with the sex to which he is attracted.

You can read Claudia’s story in the Guardian, of all places:
Claudia’s Story
Modern routes to inculcate Gender Dysphoria in our kids are linked to the rise of the internet and confessional content by transgender influencers. Binge watching this content is something many detransitioners say fostered a desire to transition. In the U.K prominent children’s organisations , such as Childline (run by the NSPCC: National Society For the Protection of Children) promote these transgender influencers in, from my perspective, a reckless fashion. This played a role for my son, in addition to the relentless homophobic bullying that goes on in our schools.

Fifteen years after Claudia’s experience no lessons have been learned. The same inadequate assessments are happening to our troubled youth, from within a captured NHS. The role of inducement and coercion is driving our kids and vulnerable adults down a tragic path.

NY Times: Product Placement
You are the product. Exhibit A. Who among us does not think this woman seemed in dire need of therapeutic help and not the surgeons knife. Yet here the New York Times are publishing this as a tale of redemption and authenticity. How Mac McClelland went from staging her own violent rape to address sexual trauma to more self-harm. What message does this send to vulnerable young women in flight from the dangers of living as a woman?
This story, coincidentally, came to my attention as I was writing this piece. We learn that the subject is an asexual with a boyfriend. They have already had a double mastectomy and their uterus has been removed. They refer to their ”native penis” sometimes called the ”clitoris”. This is not science It’s a belief system. They talk about how they want to retain their vagina but also it’s a case of ”penis or death” . 👇

The quasi-religious language is common in the phallioplasty files, as covered by the YouTuber Exulansic. The Gender surgeons are the priest class, administering the trans rites required by Gender Jesus, to their willing disciples. It’s a new religion fuelled by the techno-barbarism of the Gender Industrial Complex. Mining profits from our bodies as if there are endless spare parts grown on a human meat farm.
Back to the article:
In a strange way the more extreme proponents of body modification, in the name of the Gender religion, seem to convince the clinicians it’s the right path for their patient. Nobody would do this to themselves unless it was right for them, would they?
Here a detransitioner speaks out, at a meeting I attended. Only when she joined a support forum for women, who had also gone through hysterectomy, did it dawn on her this was a uniquely female experience.

Some of the people at the detransitioners meeting were themselves involved in the Gender Industrial Complex. If I had sat in a room with young Lesbians who, between them, regretted testosterone, double mastectomies, hysterectomies and ovary removal, I would have left the Industry immediately. Yes, I mean you, Stuart Lorimer: Seen below with Susie Green accompanied by an excerpt from an interview he gave. Our mutilated kids are to fund Stuart’s pension plan.
Excellent question below. Do the NHS and Gender Clinics think about detransitioners when they dish out drugs to our teenagers? Or the Puberty Blockers they are giving to 10 year olds? Personally I would not sleep at night.

Here Bernadette Wren acknowledges the political pressure from third sector organisations (Lobby Groups) on services like GIDS. Mermaids is a pernicious influence on the Gender Industrial Complex. Mermaids CEO, Susie Green, arranged to have her 16 year old son undergo sexual reassignment surgery, in Thailand. Her career seems driven by a desire to justify this decision. Bernadette may also wish to divert attention from the role the Tavistock Gender Identity Service played. She worked there when they introduced the Dutch Protocol and began putting children, as young as 10, on Puberty Blockers.

Here is a reminder of what Bernadette told the Parliamentary Inquiry on Transgender Equality. This does not sound like a reluctant, cautious clinician. It sounds like a statement from a social justice warrior . “It is a social revolution that many of us really fought for and wanted around sex and gender”.

The admission that they were heading in an unknown direction! The breathtaking hypocrisy of blaming the appearance of so many natal females, at the Tavistock, on the failures of feminism! Whilst, simultaneously, facilitating this body hatred with mutilating surgeries!
The paucity of research into psychological underpinnings for the presence of Gender Dysphoria is an international scandal. This is compounded by the failure to follow up those patients who accessed surgical intervention. For me, the moment you advocate for surgery, to resolve a mental health issue, you have failed as a Clinical Psychologist and betrayed your client at their most vulnerable.

This on breast binding. Its the same old bodily hatred that used to be manifested as anorexia. In this country we have official advice to watch out for girls whose families may encourage breast ironing. At the same time corporate enterprise Lush can offer free breast binders as a marketing campaign!

No, Bernadette, you most definitely are not supporting creative expressions of masculinity or femininity. You are telling our gender non-conforming kids they may be born wrong and normalising making yourself a medical patient for life! If you really believe this is what your life’s work was about you are deluded. I would say get some help but where would you go? This is a self-serving justification that reframes the perpetration of extreme harm as necessary and virtuous.
{The Destroy Your Binder video has been removed from YouTube but you can read a transcript on Kat’s Tumbler.}
Destroy Your Binder
Next up Kirsty addresses a response which extols the virtue of a mastectomy for one patient who reports positive feelings about their surgery. This article is not open access but is here:
https://acamh.onlinelibrary.wiley.com/doi/full/10.1111/camh.12343

There are many positive accounts on YouTube celebrating getting your, healthy, breasts removed. To which I say “come back in ten years”. I don’t doubt there may be some who never regret this surgery but there are many detransitioners, as related below, who do and others who find it triggers them on to the next set of surgeries; which suggests it was not the panacea they were sold.

Here Ken Zucker uses the word “iatrogenic” for which 👏👏. The social transition of children and its impact on future medicalisation needs researching. Does it foreclose any reconciliation with birth sex? He also rightly comments on the escalating desire for mastectomy which often follows painful breast-binding. He also reports that bodily rejection migrates to the genitals, post mastectomy.

The article ends with

The victims of this modern, mass delusion, are the most vulnerable in our society. Bullied gay youth, girls with eating disorders, autistic kids and kids in local authority care. All groups over-represented at Gender Clinics.
Why has it taken so long to investigate the harms perpetrated primarily on young females in the past decad? The featured image on this post is of a 13 year old girl posing with her surgeon who advertises on TikTok, populated by malleable kids/teens. She calls herself Dr Teetus Deletus to market her services to the youth market.
I do this full-time and have no income. If you want to support my work, and can afford to do so, here is one way.
Researching the impact of Gender Identity Ideology on women & girls as well as the consequences for Lesbians, Gay males and autistic kids. I do this full time and have no income. All my content is open access and donations help keep me going. Only give IF you can afford. Thank you to my generous donors.













































































































































{kind=link}