
Long overdue post on the new gender clinic and who is involved. First up is Aidan Kelly who has his own series on this blog. Someone been busy removing links to existing YouTube content so there may be missing links. Here is a link to his series.
Gender Plus now has its own YouTube channel which you can access here.
I have chosen to look first at an interview on the Times Radio channel, in the hope it interrogates Dr Kelly, rather more than the Gender Plus channel, which is really an extended advert for their profit making venture. Here is a link 👇
Kelly is asked about the closure of the Tavistock, the controversy about using puberty blockers, high rates of referrals from the autistic community and detransitioners. Unfortunately he was not asked about why there are so many referrals to Gender Clinics, who are same sex attracted or from the looked after sector (Foster kids) or are adopted. This is a shocking omission.
Before I get into the meat of the interview someone at Gender Plus made a revealing choice of name. There is a book of the same name which is about a gay man who was successfully, he claims, converted into a happily, heterosexual, married man. I could not resist including this as Gender Plus are, indeed, in the business of converting self hating, gay men into a facsimile of a heterosexual woman. Surely the brand manager would have searched this before they chose that name? And note the email address.



( I checked companies house and husband and wife team have a company, now dormant, called Gender Plus Ltd. Gender plus have a company called Gender Plus Healthcare Ltd which lists Kelly as the sole director.)
Kelly does some serious P.R. for the new clinic trying desperately to differentiate their “offer” from the discredited Tavistock; this despite employing quite a few ex Tavistock personnel, in addition to himself. He pays lip service to respecting and including parents, “where appropriate”; claims that clients will be seen at least six times over a six month period and avoids the prescription of puberty blockers, for under 16s. He claims that there will be no pre-determined outcomes and clients who are too certain will be questioned; whilst still validating all gender identities. He acknowledges detransitioners and “gender critical” perspectives claiming he takes a middle ground. So far so good but let’s look at some of his pronouncements and omissions. This quote gives a good idea about the kind of interrogation potential “trans” patients will get.

Dr Kelly is a psychologist by training. He is also a member of W.P.A.T.H (A lobby group for “transgender” medicine and the British Association for Gender Identity Specialists.)


Gender Affirming Care?
He denies that he is a proponent of “gender affirmative” care but also claims all identities are validated by Gender Plus. I presume the client would be granted opposite pronouns, or neo-pronouns as per the client’s wishes. No doubt Dr Kelly considers this to be a matter of respect so I would love to see how he is able to explore the possibility that his client may simply be “cisgender”, after he has accepted this framing? It’s important to emphasise that one of these “identities” can involve lifelong dependence on pharmaceutical interventions and possible surgeries. In what other situation would the medical profession actively collude with a desire which leads to being a lifelong medical patient? Speaking as a parent I am unashamedly in favour of the identity that does not promote iatrogenic harm.

Kelly’s position is patient led so, ultimately, if the person persists in the desire for these medical interventions, he will support them. If the patient feels this is the best way of living their life then Dr Kelly is happy to offload the responsibility to the patient.

The debate on “patient” led care is occurring outside of the issue of “transgender” care. Some commentators embrace patients as “customers” and are averse to what they see as the paternalism of the medical profession. Others have written about the need for Doctors to take on the diagnostic role and development of a treatment pathway, citing risk of over diagnosis and over treatment, if totally reliant on the patient’s wishes. Dr Kelly is not a medical doctor but he is willing to take risks with other people’s health bodies. He justifies this with a concept he calls “safe risks”. How brave and self sacrificing is he?

Explosion of referrals to the Tavistock.
In the context of this branch of, so called, medicine the interviewer asks about the explosion in referrals to the Tavistock over recent times. This graph, from Transgender Trend, captures the scale of the increase since 2009.

Dr Kelly candidly admits that nobody knows why this has/is happening. He shows little curiosity about this expanding market, which now consists mainly of the, newly emergent, phenomenon of teenage girls; the cohort historically most susceptible to social contagion.

Kelly simply accepts this, relatively, new phenomenon as a genie that has escaped the bottle. After all this is how he makes his living.

Neurodivergent kids.
Asked about the high rates of autistic kids referred to Gender Clinics, Kelly seems to detect a whiff of ableism and is keen to champion bodily autonomy for autistic kids. Later in the same interview he explains that autistic patients have difficulty following social norms and they are more resistant to any social pressure to conform to sex stereotypes! That, he implies, might be part of an explanation. He could reflect on black and white thinking, common neuro divergent kids, and how common it is to be hyper focused and obsessional rumination once an idea appeals. He seems, to me, to seek the explanation more likely to comply with his business model.

Detransition.
Kelly is asked about detransition and the interviewer reads two, devastating, accounts from detransitioners Ritchie Heron and Sinead Watson. Kelly feigns ignorance about the testimony of Heron, even though he has had widespread media coverage and is taking legal action over his “transition”. Here is what he has to say about these, harrowing, accounts.

He seems quite sanguine about the risks and even admits his own patients may be the detransitioners of the future.

Nobody has a crystal ball, after all. Ironically the approach here sounds about as scientific as mystic meg. Not the standard I would expect for evidence based medicine.

Dr Kelly appears not to have done any up to date research on “detransition” he quotes a figure of 1% based on an unspecified Adult Clinic in London. He doesn’t have the research to hand…but he thinks and believes he helps the people he sees. He later concedes it’s a poorly researched area. 👇


For anybody that is interested I have done a series on detransition and the one from Cambridge, flawed as it is, conceded we are likely underestimating regret rates. It’s shaming that Dr Kelly doesn’t appear to keep himself up to date. Here is a clip on the Cambridge study into regret rates. Even they said it was 6.9% and I would argue their methodology tended to exclude people from being classified as having “regret”

The Cambridge article on detransition link below. 👇
Detransition: Cambridge Study (2)
Puberty Blockers
Gender Plus has decided that the prescribing of puberty blockers, for those under 16,is too much of a contentious area, at present. They are however still going to “treat” children whatever that means.

At the same time Kelly claims to have evidence, albeit anecdotal of their successful use.

Finally…
The interviewer asks what working in this field is like for Kelly. He explains he is a true believer and clearly doesn’t share my view of what makes an extremist.

Next up, I will look at some of the others players at Gender Plus.
You can support my work by taking out a paid subscription to my substack or donating below. All donations gratefully received and they do help me cover my costs and also to keep content open for those not able to contribute. (I will add other methods as soon as I have figured it out. 😉)

Researching the history and the present of the “transgender” movement and the harm it is wreaking on our society.
£10.00























 He explains that referrals in 1989 numbered three, by 2010 rates were doubling annually and, by 2016/17, they hit 2000. At the same time the sex ratio of referrals had completely inverted to comprise predominantly females. 75% female whereas only a decade earlier the service would have catered to 75% males. Aiden is puzzled by this growth and appeals to his audience for help:
He explains that referrals in 1989 numbered three, by 2010 rates were doubling annually and, by 2016/17, they hit 2000. At the same time the sex ratio of referrals had completely inverted to comprise predominantly females. 75% female whereas only a decade earlier the service would have catered to 75% males. Aiden is puzzled by this growth and appeals to his audience for help: 



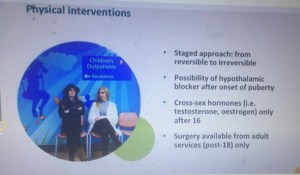 The first stage is Puberty Blockers. As of March 2018 these were still being described as a “pause”. This has been a contested statement for years. I have blogged about this in earlier posts. Here:
The first stage is Puberty Blockers. As of March 2018 these were still being described as a “pause”. This has been a contested statement for years. I have blogged about this in earlier posts. Here: 
 they are fully reversible and only pause puberty. This would now appear to be recognised as false. Note also that, as of March 2018, the Tavistock protocol is that children be allowed to go through a partial puberty, as he explicitly says in this second clip This is important for young people to get an idea, not just of their Gender, but also their Sexuality. Below, Dr Aiden, expands on this important issue. He concedes a few important points.
they are fully reversible and only pause puberty. This would now appear to be recognised as false. Note also that, as of March 2018, the Tavistock protocol is that children be allowed to go through a partial puberty, as he explicitly says in this second clip This is important for young people to get an idea, not just of their Gender, but also their Sexuality. Below, Dr Aiden, expands on this important issue. He concedes a few important points.  The lack of research. The experimental nature of the treatment. The fact that many of them won’t persist in a wish to change sex. Here Dr Day uses an estimate of a 50/50 split between those who would persist and desisters. I have done many blogs looking at rates of desistance and, whilst the research is contested, a figure of 80% would seem to have more validity than a split of 50/50.
The lack of research. The experimental nature of the treatment. The fact that many of them won’t persist in a wish to change sex. Here Dr Day uses an estimate of a 50/50 split between those who would persist and desisters. I have done many blogs looking at rates of desistance and, whilst the research is contested, a figure of 80% would seem to have more validity than a split of 50/50.

 could be available as young as 10! The current , public, protocol published by the Tavistock has an age limit set at age 12.
could be available as young as 10! The current , public, protocol published by the Tavistock has an age limit set at age 12. I would never agree to any treatment that I thought would imperil my child’s sexuality. I fear many affirming parents are not in full posession of the facts and are terrified by the spectre of suicide. They should not be
I would never agree to any treatment that I thought would imperil my child’s sexuality. I fear many affirming parents are not in full posession of the facts and are terrified by the spectre of suicide. They should not be 








 The speed of the change has clearly taken the clinic by surprise. The societal embrace of the “Transgender Child” has swept our society at breakneck speed. Only a decade ago some of the practices we are seeing today would have been unthinkable.
The speed of the change has clearly taken the clinic by surprise. The societal embrace of the “Transgender Child” has swept our society at breakneck speed. Only a decade ago some of the practices we are seeing today would have been unthinkable.


