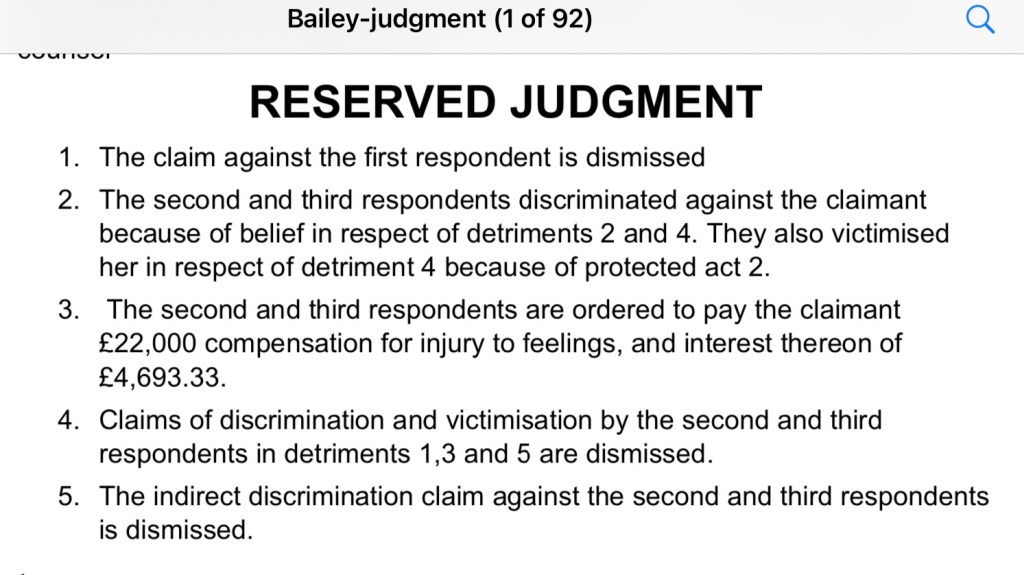
Sonia Appleby is the safeguarding lead for the Trust that houses the Tavistock, or Gender Identity Development Service (GIDs). Sonia bravely took her employer to an Employment Tribunal ; which she won. You can read the full judgment below.
Ms_S_Appleby__vs___Tavistock_and_Portman_NHS_Foundation_Trust
The full judgment contains many of the red flags that, no doubt, form part of the background to the closure of the Tavistock (G.I.Ds).
Sonia Appleby was the safeguarding lead for the NHS Trust which, until recently, housed the Gender Identity Service. Sonia’s case centred on the six issues she raised under the whistleblower policy and whether she suffered detriment as a result. She won her case and was awarded £20,000 in compensation.

In order to determine the case many staff were interviewed and some were cross examined.


Matt Bristow was not cross examined but his witness statement, on behalf of Sonia Appleby is on the public record. 👇 This encapsulates his concerns. Gay Conversion Therapy, in a nutshell.


Sonia was in the middle of an internal dispute between staff at the Tavistock about the best way to treat their referrals. Some staff believed in an innate “gender identity” where the children know best and it’s the clinician’s role to affirm their “authentic self”. This is an ideologically predicated perspective. Others were concerned about the other potential influences on the child’s internal belief system. Autism, same sex attraction, backgrounds of abuse or other trauma were present in a lot of the children. Some clinician were worried about the role of social media and the explosion of “trans” in the media fuelling a social contagion. Appleby was in the eye of the storm attempting to enforce child safeguarding in the midst of this, highly charged, environment.

The service had seen a steep rise in referrals, from mainly male it had switched to 76% female, waiting lists were long and the first court case, questioning the use of “affirmation” only had already been heard. This was the case of Keira Bell, a case I cover here:
It was not just internal strife that bedevilled the service. The issue had become highly politicised with women’s groups springing up to contest the attacks on female only spaces by trans activists. Controversial lobby group, Mermaids, was garnering a lot of media attention and the promotion of “transgender” children was peddled across the U.K media. Accusations of “transphobia” were rife.

Sonia Appleby had experience as a social worker and a psychoanalytical psychotherapist and was named lead for safeguarding children for the Trust. By June 2016 she was raising the alarm at the rise in referrals and the increasing workloads. She also noted deficiencies in record keeping. Staff were also raising concerns about the role of a private practitioner who had entered the fray.

Dr Webberley has been suspended from practice for a number of years, her husband, who worked alongside her, was actually removed from the medical register this year. G.I.Ds staff were beginning to see children who had not only socially “transitioned” but had already accessed puberty blocking drugs from private practitioners such as Webberley.
Dr Carmichael’s response to this requested meeting is described as “interesting” in that she expressed concern that she “was unsure the agenda here”. She claimed she was simply wondering what the agenda was for the meeting. The tribunal was not convinced by this explanation”.

This was Sonia Appleby’s first protected disclosure. Mermaids, Rogue Medics and tensions within the team.

The second list of concerns is even more damning. Again Dr Webberley features; as does the number of gay kids presenting as “transgender”; parental encouragement of their child’s identity; and Dr Carmichael’s unwillingness to listen all feature.

There emerged some confusion about who was taking these issues forwarded and during a flurry of emails Appleby became aware that Dr Carmichael resented her being approached by her own staff. At this point a Garry Richardom is brought on board to play a role in safeguarding internal to G.I.Ds. This relationship gets off to a rocky start because he objects to her use of Jimmy Savile as a warning to the service.

Sonia explains this was something she routinely did to embed safeguarding in the service by using the example of Jimmy Savile who is the most high profile example of the NHS failing to spot /act upon a major safeguarding risk.
By 2018 a group of ten staff raised concerns with Dr David Bell. The claimant also raised another list of concerns raised by a staff member. Again the issue of homophobic parents raises its ugly head and a lack of understanding of the effects of puberty blockers.

She then conducted an audit of safeguarding referrals and noted that the rate of referrals was very low at G.I.Ds compared to other areas of the Trust. Appleby felt relations with Dr Carmichael were strained she was cast as someone asking “awkward questions”. At the same time Dr David Bell began interviewing staff and preparing his own report documenting concerns. This report was damning and would be leaked to the press. Once again homophobia is identified as an issue as well as the “excessively affirmative” attitude of staff who were seen as unable to withstand pressure to medically intervene.

Dr Carmichael’s response appears defensive.

At this point the claimant needed to establish a working relationship with a Dr Sinha who joined the service. This got off to a rocky start as he was briefed that she did not like to be managed and worked too independently, he reported that he found her argumentative but was unable to provide examples, to the tribunal, of incidents that led to this conclusion. There follows some exchanges that illustrate that Sonia Appleby was regarded with suspicion even when collecting data which was required for her job.
There followed a fifth protected disclosure based on the exit interview of Dr Matt Bristow. By this time Sonia Appleby is regarded with suspicion across the service and evidence is brought to the tribunal that staff were being discouraged from bringing safeguarding concerns to Sonia. Email trails who that staff were complaining about her “insubordination” and Dr Sinha embarks on disciplinary proceedings resulting in a letter being placed on her file. The tribunal found the way this was handled to be unfair to the claimant. Dr Sinha was found to be hostile and “punitive”.

Sonia was labelled as “not on side” by Dr Carmichael and evidence is presented illustrating that Sonia was safeguarding issues were not being referred, to her, by staff.

The tribunal concluded that there was a message being communicated that Appleby was hostile to the service and being cut out of issues in relation to her role as child safeguarding lead.

The tribunal found that the claimant had suffered detriment and an award of £20,000 was made. The picture that emerges is of a service riven with tension and suspicion where raising safeguarding concerns was viewed as a hostile act. The recurrent theme is one of homophobia which echoes my own experience. Our gay youth are poorly served/actively harmed by this service, in my view. The removal of the service from the Tavistock was long overdue.
You can support my work here. All contributions gratefully received.

Researching the history and the present of the “transgender” movement and the harm it is wreaking on our society.
£10.00























































 Cue cries of “transphobia” for wishing to be free of all genders of penis when women are in intimate spaces.
Cue cries of “transphobia” for wishing to be free of all genders of penis when women are in intimate spaces.


 Well he would wouldn’t he? Fetishising a female identity is pretty much the essence of the movement but I would say that wouldn’t I?
Well he would wouldn’t he? Fetishising a female identity is pretty much the essence of the movement but I would say that wouldn’t I?







 Article, in full, here
Article, in full, here 
 Will I draw fire from Social Justice Warriors if I appropriate the Chinese Curse “May you live in interesting times”. Women, in the UK, are indeed living in a cursed place.
Will I draw fire from Social Justice Warriors if I appropriate the Chinese Curse “May you live in interesting times”. Women, in the UK, are indeed living in a cursed place.








 Whilst there could be a progressive case for reviewing the law covering sex by deception (I am thinking of
Whilst there could be a progressive case for reviewing the law covering sex by deception (I am thinking of 
















 Now the concept of an “innate gender identity” is treated as a medical, but not a mental health, condition much of this defence would, presumably, be moot. A genuinely held belief that you are the opposite sex doesn’t change biological reality. If someone has a Gender Recognition Certificate there are privacy laws protecting that information. They are to be treated as if they are the opposite sex. Is there any protection, other than sex by deception, for women, or men, deceived in this way? Extreme activists would say there is no deception. They would argue they literally are the sex they say they are. That there is a deeply held conviction I can accept, that I should have to share it is the sticking point.
Now the concept of an “innate gender identity” is treated as a medical, but not a mental health, condition much of this defence would, presumably, be moot. A genuinely held belief that you are the opposite sex doesn’t change biological reality. If someone has a Gender Recognition Certificate there are privacy laws protecting that information. They are to be treated as if they are the opposite sex. Is there any protection, other than sex by deception, for women, or men, deceived in this way? Extreme activists would say there is no deception. They would argue they literally are the sex they say they are. That there is a deeply held conviction I can accept, that I should have to share it is the sticking point.


 In addition to marrying three times, and fathering 7 children, the appellant has a criminal history. In 2011 they were sentenced to eight years in prison. The judge makes it clear that the appeal is not concerned with the criminal offences. Also the papers detailing the offence were not included and, moreover, that this was not relevant to the “wider public debate”.
In addition to marrying three times, and fathering 7 children, the appellant has a criminal history. In 2011 they were sentenced to eight years in prison. The judge makes it clear that the appeal is not concerned with the criminal offences. Also the papers detailing the offence were not included and, moreover, that this was not relevant to the “wider public debate”.  For the terminally curious. Here is a brief allusion to the offence so you can judge for yourself whether it is “relevant”
For the terminally curious. Here is a brief allusion to the offence so you can judge for yourself whether it is “relevant” 







 The relationship with Webberley doesnt seem to persist and another doctor appears. The next Doctor issues a report which is submitted, in redacted form, the the Gender Recognition Panel. This doctor again refers to Ms Jay’s personality disorder and maladaptive coping mechanisms but does diagnose Gender Dysphoria. The diagnosis leads to the recommended treatment (gender reassignment) to resolve the psychiatric issues. Nobody asks whether craving Gender Reassignment is another maladaptive coping mechanism. That would be transphobic, just in case any of you are thinking that now! Gender Dysphoria has been rebranded as an “identity” not a mental health issue, it’s now a slur to suggest this. As an aside this expert also recommends consideration is given to moving the prisoner to the female prison estate. In March 2016 the application for a GRC was turned down. The doctor disappears from the case.
The relationship with Webberley doesnt seem to persist and another doctor appears. The next Doctor issues a report which is submitted, in redacted form, the the Gender Recognition Panel. This doctor again refers to Ms Jay’s personality disorder and maladaptive coping mechanisms but does diagnose Gender Dysphoria. The diagnosis leads to the recommended treatment (gender reassignment) to resolve the psychiatric issues. Nobody asks whether craving Gender Reassignment is another maladaptive coping mechanism. That would be transphobic, just in case any of you are thinking that now! Gender Dysphoria has been rebranded as an “identity” not a mental health issue, it’s now a slur to suggest this. As an aside this expert also recommends consideration is given to moving the prisoner to the female prison estate. In March 2016 the application for a GRC was turned down. The doctor disappears from the case.

 In August 2017 the Gender Recognition Panel again turned down the application. They expressed doubt about the credibility of the supporting evidence and , in particular that of Dr Pasteracki. They cast doubt on evidence supplied by the claimant.
In August 2017 the Gender Recognition Panel again turned down the application. They expressed doubt about the credibility of the supporting evidence and , in particular that of Dr Pasteracki. They cast doubt on evidence supplied by the claimant.


 The advocate for the claimant also shares this interesting nugget about GRC applications. Less than 5% are refused its designed to be
The advocate for the claimant also shares this interesting nugget about GRC applications. Less than 5% are refused its designed to be  You have to admire the fancy footwork of the Legal team. Ms McCann that the prisoner met the legal standard and that this Judge had the authority to award the Gender Recognition Certificate himself. Is it possible that some Judges are a tad vain and like to set precedents? Does the advocate absolutely know this fact about male vanity? [
You have to admire the fancy footwork of the Legal team. Ms McCann that the prisoner met the legal standard and that this Judge had the authority to award the Gender Recognition Certificate himself. Is it possible that some Judges are a tad vain and like to set precedents? Does the advocate absolutely know this fact about male vanity? [ To demand that I accede to your self-identity which may contradict my sex recognition skills springs from a totalitarian impulse. Chances are I will see your sex and if you walk behind me, late at night, I will react accordingly.
To demand that I accede to your self-identity which may contradict my sex recognition skills springs from a totalitarian impulse. Chances are I will see your sex and if you walk behind me, late at night, I will react accordingly.


 I will leave you with this question. In making these determinations the Judge has to have regard to the individual’s Human Rights but also the wider rights of the Community. Are we well served?
I will leave you with this question. In making these determinations the Judge has to have regard to the individual’s Human Rights but also the wider rights of the Community. Are we well served?




 Key intersex advocates are keen to highlight that disorders of sexual development are not an “identity” and have no place in the Transgender “debate”. People who are intersex , sufferers of disorders of sexual development (DSDs), do not have a transgender “identity”. They have a medical condition that, for some, can be quite distressing. This case makes a clear distinction; which activists have tried to blur for political reasons You can read more about this here, by Claire Graham, who writes from her own experience.
Key intersex advocates are keen to highlight that disorders of sexual development are not an “identity” and have no place in the Transgender “debate”. People who are intersex , sufferers of disorders of sexual development (DSDs), do not have a transgender “identity”. They have a medical condition that, for some, can be quite distressing. This case makes a clear distinction; which activists have tried to blur for political reasons You can read more about this here, by Claire Graham, who writes from her own experience. 




 He is right to show such compassion. However kindness does not override the need to make legislation that is workable and, crucially, doesn’t dismantle protections for another vulnerable group. The judge does go on to raise the difficult judgements this would lead the law to make. Here he asks the burning question now dividing opinion in the UK. “Should self-perceived gender be recognised”.
He is right to show such compassion. However kindness does not override the need to make legislation that is workable and, crucially, doesn’t dismantle protections for another vulnerable group. The judge does go on to raise the difficult judgements this would lead the law to make. Here he asks the burning question now dividing opinion in the UK. “Should self-perceived gender be recognised”. 
 I suspect this would have been dismissed as the “slippery slope” argument. Well its not a slippery slope now. We are skiing down the slope like Eddie The Eagle without his glasses. (I do hope I got the pronouns correct). Yet here we are. Male bodied people i.e. men, are identifying as women and housed in female prisons and, we now know, allowed to demand to be on female wards in our hospitals.
I suspect this would have been dismissed as the “slippery slope” argument. Well its not a slippery slope now. We are skiing down the slope like Eddie The Eagle without his glasses. (I do hope I got the pronouns correct). Yet here we are. Male bodied people i.e. men, are identifying as women and housed in female prisons and, we now know, allowed to demand to be on female wards in our hospitals. 
 In the end the Lords ruled against the appellant. Parliament were just about to legislate for Gender Recognition to be decided, in law. Sadly they seem now to have disregarded this astute advice.
In the end the Lords ruled against the appellant. Parliament were just about to legislate for Gender Recognition to be decided, in law. Sadly they seem now to have disregarded this astute advice.  Whether or not sexual reassignment surgery will, eventually, be deemed the wrong “treatment” the fact remains that society has colluded in the development of a “transsexual” community. Society now needs to resolve how they are accommodated. Gender Reassignment also needs a more critical evaluation. Is it a mechanism to sidestep the central issue: Why are so many men are in flight from masculinity? Why are males so threatened by feminine men? Why are we allowing men trapped in male bodies to redefine what it is to be a woman? These are big questions and few of our media are covering in any meaningful way.
Whether or not sexual reassignment surgery will, eventually, be deemed the wrong “treatment” the fact remains that society has colluded in the development of a “transsexual” community. Society now needs to resolve how they are accommodated. Gender Reassignment also needs a more critical evaluation. Is it a mechanism to sidestep the central issue: Why are so many men are in flight from masculinity? Why are males so threatened by feminine men? Why are we allowing men trapped in male bodies to redefine what it is to be a woman? These are big questions and few of our media are covering in any meaningful way.


 Before we get into the complainants distress about lack of breast growth the NHS does offer genital reassignment surgery (GRS/SRS) for the condition of Gender Identity Disorder. This is because it has been accepted that Gender Dysphoria, in fe/males, presents as an extreme discomfort with reminders of your biological sex. The PCT make the treatment they will fund abundantly clear. The Complainant has not sought any genital surgery.
Before we get into the complainants distress about lack of breast growth the NHS does offer genital reassignment surgery (GRS/SRS) for the condition of Gender Identity Disorder. This is because it has been accepted that Gender Dysphoria, in fe/males, presents as an extreme discomfort with reminders of your biological sex. The PCT make the treatment they will fund abundantly clear. The Complainant has not sought any genital surgery. So let’s just take a moment here. This person has been diagnosed as “Transexual” since 1996. It’s now over a decade later and, despite Gender Dysphoria, the offer of genital reassignment surgery, has not been taken up. One would have thought the most male thing about a man was his penis and yet, instead of pursuing this, we have multiple court cases to get “breasts”!
So let’s just take a moment here. This person has been diagnosed as “Transexual” since 1996. It’s now over a decade later and, despite Gender Dysphoria, the offer of genital reassignment surgery, has not been taken up. One would have thought the most male thing about a man was his penis and yet, instead of pursuing this, we have multiple court cases to get “breasts”! 
















