
Since writing about the Birmingham Trans Policy, an informant told me there was a longer document called The Procedure for supporting Transgender People. I decided to have a look and see what it adds!
Here is the procedure.
Procedure for Supporting People who are Transgender UHB.PDF
You can read part one below. I will try not to duplicate what was covered in the policy.
I decided to look at hospital policies around single sex wards, after the revelation a woman was not only raped on an NHS ward, but then gaslit by the hospital. Imagine telling a victim “you were not raped because there were no men on the ward!”. There were. One of them was a rapist. If you are not aware of this incident I covered it here:
This document provides lots of guidance about ensuring a ”trans-identifying” person’s sex remains private. This covers staff and patients which is why staff are colluding with the idea the man, you can clearly identify is a man, is really a woman, they are compelled to hide this information. If the patient /staff member has a Gender Recognition Certificate this is enforced by the law.
This is what the Gender Recognition Act says about maintaining privacy. As you can see any disclosure of the ”protected information” attracts an unlimited fine.


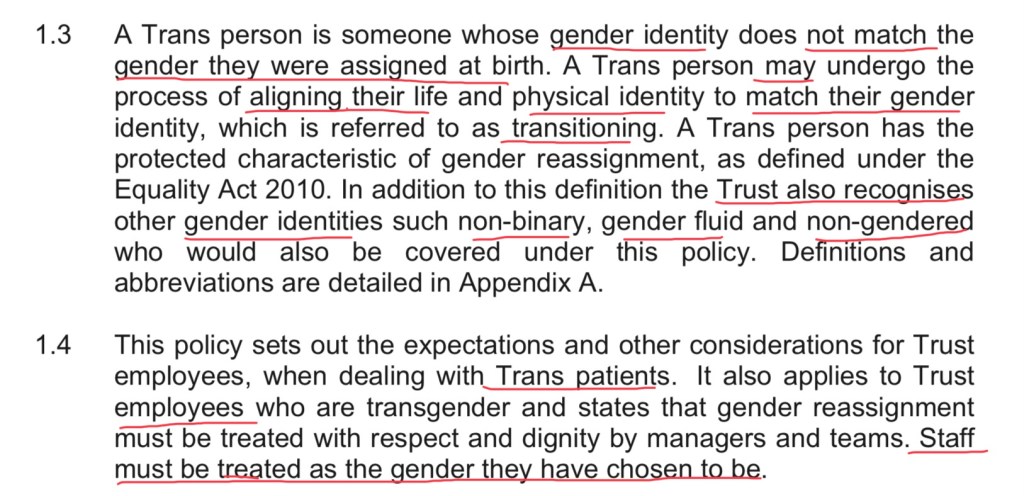
Bearing in mind no medical treatment is required. A fully intact male could identify as a woman, non-binary, gender fluid etc etc and Birmingham hospital will act on a self-ID basis. This means they allow males on ”single sex” wards purportedly for females. They are allowed to use female toilets and changing rooms.
The implication for medical notes and treatment seem to be incredibly ill thought out. Clinicians are instructed to record a male as a woman. No reference should be made to the patients biological sex, unless it is deemed relevant.

It is worth pointing out that there is an entire medical field on sex specific medicine which aimed to redress the assumption that males are the default patient. Article below:
Staff are warned to ask the patient’s permission to record any issue pertinent to their sex. What if the trans-identifying person is so deeply immersed, in their fiction, they can’t face anyone knowing? There are prominent trans activists, who are male, who claim to be Adult Human Females. India Willoughby even claimed to have a cervix. 🤦

Some of these people seem to need protecting from themselves, not enabled.

As in the policy, the trans person is to be allowed to decide which sex they wish to be allocated. The women get no choice. Staff are told it is not acceptable to make use of side-rooms. This is by far the best resolution and hardly something to complain about, unless your motivation is a desire to be validated by hospitalised women.
The procedure also makes it clear that treatment can be withheld and patients /visitors can be barred if they behave in a discriminatory manner. Does this include correctly sexing a man and objecting to being places on a mixed sex ward?

How do you foster good relations between the people with the protected characteristic of SEX (everybody) when you are forcing the female people to share space with males? They even have the cheek to head this Single Sex. Again unisex facilities are rejected as an option, for the trans-identifying person, but women are forced into mixed sex spaces. The common sense solution is rejected because this is about women being forced to act as, unpaid, validation aids for dysphoric males /entitled men.

Here is what the Trust claims are examples of unlawful discrimination. Some of this is ethically dubious, compelled speech and it is doubtful whether these would be found unlawful now gender critical beliefs are protected in law.

Here are some case studies: Here it is made clear that women will be forced to accept a man on their ward. Rachel is now ”female”. 🧐

Here they make it clear misgendering will be treated as a disciplinary offence. We have gone way beyond polite concessions. From #BeKind to #BeCompliant.

There follow two examples where a patient refuses to be treated by a “Tranny”. The use of this pejorative language allows the Hospital to refuse to provide an alternative person to treat them. I notice they do not use an example of a female, in respectful language, asking for intimate care to be provided, by someone of the same sex. This is, I would suggest, is done quite deliberately.
Finally a note on who Birmingham thinks are appropriate sources of guidance on this topic. All Trans Lobbyist who take extremist positions. Birmingham are a Stonewall Champion, last time I checked.

I can relate 👇

You can support my work here. We need to dismantle this dangerous ideology one expose at a time.

Researching Gender Identity Ideology. Examining it’s impact on women’s rights and the health of our gay teens.
£10.00



















































 Before we get into the complainants distress about lack of breast growth the NHS does offer genital reassignment surgery (GRS/SRS) for the condition of Gender Identity Disorder. This is because it has been accepted that Gender Dysphoria, in fe/males, presents as an extreme discomfort with reminders of your biological sex. The PCT make the treatment they will fund abundantly clear. The Complainant has not sought any genital surgery.
Before we get into the complainants distress about lack of breast growth the NHS does offer genital reassignment surgery (GRS/SRS) for the condition of Gender Identity Disorder. This is because it has been accepted that Gender Dysphoria, in fe/males, presents as an extreme discomfort with reminders of your biological sex. The PCT make the treatment they will fund abundantly clear. The Complainant has not sought any genital surgery. So let’s just take a moment here. This person has been diagnosed as “Transexual” since 1996. It’s now over a decade later and, despite Gender Dysphoria, the offer of genital reassignment surgery, has not been taken up. One would have thought the most male thing about a man was his penis and yet, instead of pursuing this, we have multiple court cases to get “breasts”!
So let’s just take a moment here. This person has been diagnosed as “Transexual” since 1996. It’s now over a decade later and, despite Gender Dysphoria, the offer of genital reassignment surgery, has not been taken up. One would have thought the most male thing about a man was his penis and yet, instead of pursuing this, we have multiple court cases to get “breasts”! 

















{kind=link}