
Domenico Di Ceglio set up the childhood and adolescent services at the Gender Identity Development Service (G.I.Ds) at the Tavistock. You can find the rest of my series, on the Tavistock, below.
To provide some background to a piece on the David Taylor report, into G.I.Ds, I did some research into the man who set up the children’s service. Domenico Di Ceglie can be seen on this YouTube of a conference contribution he made. 👇
This is the title of that talk. Transgender , Gender and Psychoanalysis, with this subtitle.

First he provides his motivation for setting up the service, he admits it was a new area for him until he encountered a teenage girl, who had attempted suicide three times and believed she should have been male. According to Di Ceglie she went on to identify as Ian and was suicidal no more. It was this patient, who wished her parents could have seen someone when she was five, that prompted the setting up of the service. Not everyone accepted this idea without question and someone raised the law of unintended consequences. In the retelling Di Ceglie seemed to think this an amusing moment. (I wonder if he is still laughing as we see more and more post ”transition” regret.)

This reminded me of a conversation I had with an adult male, who self-describes as a ”transsexual”; he observed that the Tavistock provided a solution that created the phenomenon. Or to use a phrase from the business world used in the Kevin Costner film, Field of Dreams:
”If you build it they will come”.

He then uses two Freud quotes and proceeds to talk about the impact of the ”uncertainty principle” in this field. This principle is actually derived from physics but it has acquired a more general use in terms of the difficulty in predicting human behaviour, or their development trajectories. I am sure there are some sound arguments for accepting this ability to tolerate ambiguity, in a therapeutic setting, but it does rather the beg the question about subjecting children as young as 10 on irreversible, medicalised, pathways. We used to accept the certainty we would grow up to be Adult Human Females or Males, needless to say this is still true.
He then introduces Pablo Neruda, the poet, from the Film, The Postman, explaining metaphors to a Greek Postman. Again, it is a perfectly charming clip, but this seems strangely whimsical when you are actually discussing serious medical interventions, in children.
John Money and Robert Stoller
Next we learn about two pioneers working in this field. John Money, for those of you who are unaware, was a pioneer in this field. He is infamous for intervening in the life of a child who had suffered a medical accident which removed his penis. David Rheimer was a twin which provided the perfect experiment in bringing him up as a, putative, girl. As, it turns out the two boys afforded access to children for Money who was subsequently outed as a paedophile. Both boys committed suicide. There is no explicit acknowledgement of the allegations against Money, only a reference to him being a ”controversial figure at the end of his life”.
Both Stoller and Money sensed the revolutionary impact of the concept of a “Gender Identity” or ”Role” which is at odds with your physical embodiment. Stoller puts it clearest here: 👇 The replacing of a subjective, sense of self, a ”gendered soul”; irrespective of your sexed body.

Money, talking in 1992, prophesied the societal revolution we are witnessing in 2022, with a reorganisation of society which is disregarding sex based rights. The obscured word at the end of this quote is ”principles”

Di Ceglie acknowledges that the ascendance of this idea has had huge, societal ramifications but, of course, there is no space to address the disproportionate impact on the female sex. He also seems quite excited about this social revolution comparing it to Copernicus who discovered that the earth rotated around the son and not the other way around. I should add that Copernicus made a discovery of fact he did not invent an unprovable theory of innate gender identity.
Brain sex #LadyBrain
In this section Di Ceglie concedes that attempts to prove a biological basis for ”gender identity’ have foundered.

At the same time he makes this astonishing claim which needs to be highlighted. He does not think we will ever have incontrovertible evidence because this is “beyond human”. The problem is we are not dealing with post-human society he is dealing with human beings. This statement looks like a nod to ”transhumanism”.

In this next section he covers the steep rise in referrals to G.I.Ds between 1989 to 2015. Most of you will be familiar with the fact we have had a 4000% increase in female patients; a complete inversion of the sex ratio as well as a dramatic lowering of the age profile. Same sex attracted youth are over-represented and not singled out for specific mention, neither is the prevalence of referrals of teenage girls with no concomitant rise of referrals of middle aged women. Surely if this was a product of more social acceptance we would see a surge in late transitioning females? Thankfully, whilst Di Ceglie shows little curiosity about this phenomenon we do have the words of his colleague, Bernadette Wren.
Cutting edge of a social revolution

Unfortunately, for us, you are literally cutting into the bodies of our children as part of this ”revolution”. Teenage girls with extreme body hatred is not new phenomenon as Wren knows very well.
Di Ceglie also uses a number of metaphors to explore his feelings about operating on the edge in terms of the Tavistock’s practices. If I were a psychoanalyst I might suggest that using metaphors, rather than grounded language conceals what he is actually enabling, perhaps even from himself. In plainer language he explains there is a fear of both action and inaction in relation to these children . There are pressures from within and without the clinic to begin prescribing puberty blockers, to children as young as 11. Some within the service wanted to limit their role to therapy, while others were keen to prescribe puberty blockers, early, in what was known as the Dutch protocol. As we now know, the latter group prevailed. Di Ceglie explores this debate by reference to Greek myths rather than saying, in plain language, the cost benefit analysis means we will sometimes treat the ”wrong” children. The correct number of children to be medicalised, for me, is zero. No child should be sterilised and have zero capacity to orgasm. You may be skeptical of this claim so I will share the words of Marci Bowers. Bowers is a surgeon and also a “trans” identified male. He performed surgery on Jazz Jennings. These children are being robbed of their sexual pleasure.

Autism
Later he will acknowledge the high number of autistic referrals and reference a theory that links this to atypical levels of testosterone in utero leading to ”masculine” brain type. My own theory, while I don’t wholly dismiss some, sex specific, biological imprint on male and female brains, is that *some* autistic girls are not as efficient at absorbing female socialisation. Conversely, I have also seen female socialisation as an explanation for why *some* autistic girls become adept at ”masking” /mimicking their peers so are often diagnosed late in life. (I will come back to Autism in a the next piece because it is a complex area. )
I will cover the rest of this YouTube in a further blog because there was more on autism and one person pushed him on the issue of high rates of referrals with same sexual orientation. I will leave you with Bob’s excellent question.
Questions
Bob Withers.
Bob asked an excellent question which goes to the heart of the matter. I have done a series on Bob’s work. (Link below).

Now we have a growing number of detransitioners the chickens may be comimg home to roost. Currently there are 35,000 members on the reddit detrans forum. It is growing at an alarming rate.
You can support my work here. Every donation helps because we are up against billionaires funding this ideology, globally. Contrary to the propaganda I am not funded by Evangelical Christians, the Far Right or Viktor Orban. I rely on donations to cover my costs but do not donate if you are on a limited income.

Researching Gender Identity Ideology and it’s impact on our gay /autistic youth, kids in care as well as the sex based rights of women and adult homosexuals, especially Lesbians.
£10.00


































































 A growing number of parents are expressing concern about the treatment of their children with Gender Dysphoria. 30% are estimated to be on the autistic spectrum and with other co-morbidities. Many are simply gay males and Lesbians. The parent’s, referred to here 👈actually managed to get a letter published in the Guardian. They also raised concerns about on-line grooming of their children into the tenets of Transgender Identity. In the UK there are now two groups of Parents who are questioning the current approach to their Gender Dysphoric children. Bayswater Support Group: Twitter
A growing number of parents are expressing concern about the treatment of their children with Gender Dysphoria. 30% are estimated to be on the autistic spectrum and with other co-morbidities. Many are simply gay males and Lesbians. The parent’s, referred to here 👈actually managed to get a letter published in the Guardian. They also raised concerns about on-line grooming of their children into the tenets of Transgender Identity. In the UK there are now two groups of Parents who are questioning the current approach to their Gender Dysphoric children. Bayswater Support Group: Twitter  I can’t stress this point enough. Once your child starts down this path they rarely go back and they will be dependent on cross-sex hormones for life to maintain this “identity”. Tragically some of the women, and men, who have de-transitioned are still dependent on synthetic hormones, for their own sex, because they had ovaries/testes removed.
I can’t stress this point enough. Once your child starts down this path they rarely go back and they will be dependent on cross-sex hormones for life to maintain this “identity”. Tragically some of the women, and men, who have de-transitioned are still dependent on synthetic hormones, for their own sex, because they had ovaries/testes removed.







 Watching Jazz Jennings , a 16 year old male, ask if an orgasm was like a sneeze
Watching Jazz Jennings , a 16 year old male, ask if an orgasm was like a sneeze 






 Yet instead of working to, therapeutically, resolve this “splitting” we are shutting this down. Only medical pathways are seen as appropriate. Clinicians are branded transphobic for a therapeutic approach.
Yet instead of working to, therapeutically, resolve this “splitting” we are shutting this down. Only medical pathways are seen as appropriate. Clinicians are branded transphobic for a therapeutic approach.












 Michael has been indomitable in his research into the use of puberty blockers on, ever younger, children. Michael is an Oxford University academic who researches social movements and ordinary people, driven to extraordinary actions. He also researches self-harm as a form of social protest. An interesting background. As you will see from his paper he was told by some woke students to Educate Himself. So he did! Here’s what he uncovered.
Michael has been indomitable in his research into the use of puberty blockers on, ever younger, children. Michael is an Oxford University academic who researches social movements and ordinary people, driven to extraordinary actions. He also researches self-harm as a form of social protest. An interesting background. As you will see from his paper he was told by some woke students to Educate Himself. So he did! Here’s what he uncovered.






 There is more information, in the public domain, about the treatment of dangerous sex offenders, than there is of children put on the same drug. Let that sink in.
There is more information, in the public domain, about the treatment of dangerous sex offenders, than there is of children put on the same drug. Let that sink in.






































 He explains that referrals in 1989 numbered three, by 2010 rates were doubling annually and, by 2016/17, they hit 2000. At the same time the sex ratio of referrals had completely inverted to comprise predominantly females. 75% female whereas only a decade earlier the service would have catered to 75% males. Aiden is puzzled by this growth and appeals to his audience for help:
He explains that referrals in 1989 numbered three, by 2010 rates were doubling annually and, by 2016/17, they hit 2000. At the same time the sex ratio of referrals had completely inverted to comprise predominantly females. 75% female whereas only a decade earlier the service would have catered to 75% males. Aiden is puzzled by this growth and appeals to his audience for help: 



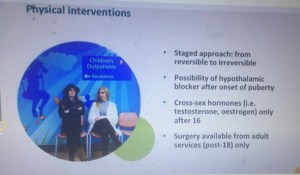 The first stage is Puberty Blockers. As of March 2018 these were still being described as a “pause”. This has been a contested statement for years. I have blogged about this in earlier posts. Here:
The first stage is Puberty Blockers. As of March 2018 these were still being described as a “pause”. This has been a contested statement for years. I have blogged about this in earlier posts. Here: 
 they are fully reversible and only pause puberty. This would now appear to be recognised as false. Note also that, as of March 2018, the Tavistock protocol is that children be allowed to go through a partial puberty, as he explicitly says in this second clip This is important for young people to get an idea, not just of their Gender, but also their Sexuality. Below, Dr Aiden, expands on this important issue. He concedes a few important points.
they are fully reversible and only pause puberty. This would now appear to be recognised as false. Note also that, as of March 2018, the Tavistock protocol is that children be allowed to go through a partial puberty, as he explicitly says in this second clip This is important for young people to get an idea, not just of their Gender, but also their Sexuality. Below, Dr Aiden, expands on this important issue. He concedes a few important points.  The lack of research. The experimental nature of the treatment. The fact that many of them won’t persist in a wish to change sex. Here Dr Day uses an estimate of a 50/50 split between those who would persist and desisters. I have done many blogs looking at rates of desistance and, whilst the research is contested, a figure of 80% would seem to have more validity than a split of 50/50.
The lack of research. The experimental nature of the treatment. The fact that many of them won’t persist in a wish to change sex. Here Dr Day uses an estimate of a 50/50 split between those who would persist and desisters. I have done many blogs looking at rates of desistance and, whilst the research is contested, a figure of 80% would seem to have more validity than a split of 50/50.

 could be available as young as 10! The current , public, protocol published by the Tavistock has an age limit set at age 12.
could be available as young as 10! The current , public, protocol published by the Tavistock has an age limit set at age 12. I would never agree to any treatment that I thought would imperil my child’s sexuality. I fear many affirming parents are not in full posession of the facts and are terrified by the spectre of suicide. They should not be
I would never agree to any treatment that I thought would imperil my child’s sexuality. I fear many affirming parents are not in full posession of the facts and are terrified by the spectre of suicide. They should not be 








 The speed of the change has clearly taken the clinic by surprise. The societal embrace of the “Transgender Child” has swept our society at breakneck speed. Only a decade ago some of the practices we are seeing today would have been unthinkable.
The speed of the change has clearly taken the clinic by surprise. The societal embrace of the “Transgender Child” has swept our society at breakneck speed. Only a decade ago some of the practices we are seeing today would have been unthinkable.















 Dr Carmichael is not happy the Tavistock are being accused of not being sufficiently affirmative. She does appear to be trying to raise awareness of the changing nature of the child referrals. Her interpretation of the parents, mentioned above. does not accord with my own perspective. Socially transitioning a three year old and then attempting to report a young child for the Hate Crime of misgendering another child! Is this the behaviour of parents who are simply being protective! If I was relaying this story, verbally, my incredulity would be at such a high pitch only dogs would be able to hear me!
Dr Carmichael is not happy the Tavistock are being accused of not being sufficiently affirmative. She does appear to be trying to raise awareness of the changing nature of the child referrals. Her interpretation of the parents, mentioned above. does not accord with my own perspective. Socially transitioning a three year old and then attempting to report a young child for the Hate Crime of misgendering another child! Is this the behaviour of parents who are simply being protective! If I was relaying this story, verbally, my incredulity would be at such a high pitch only dogs would be able to hear me!








{kind=link}